News Commentary
This is our response to a request for feedback from the public regarding the APA’s guidelines for trans and nonbinary-identified people. A complete copy of “Guidelines for Psychological Practice With Transgender and Gender Nonconforming People” can be found here and comments are received until 9/30/20:
Guideline 1. “Psychologists understand that gender is a nonbinary construct that allows for a range of gender identities”
This is an ideological statement. How is the APA defining gender? There is no universal agreement gender should be defined as something subjective with limitless variations believed by others. Very few people in the human population experience gender incongruence. Declaring all of gender to be a “nonbinary construct” is an overstatement. The APA may choose to engage this recently popularized language (mostly with roots in postmodern gender studies in academia) that values subjective experience over the scientific method, but a more grounded way to phrase this is:
“Human beings are a binary, sexually reproducing species with some intersex conditions that still fall under male & female. While males & females have differing bell curves for many traits, they overlap, & it is normal to have females who fall into ranges closer to male averages & vice versa. Some individuals experience incongruence with their biological sex due to factors that research indicates are both biological & environmental. Gender dysphoria is a spectrum.”
Word choice by the APA is important to your organization’s image & mission. Does the APA want to be a science organization or one that uses language derived from activist circles & identity studies in academia whose proponents often don’t engage their ideas in rigorous scientific discourse? There have always been gender outliers. That isn’t evidence the concepts & language used in current gender identity activism are all positive for mental health & society at large. Many people have adopted a myriad of identities (belief one is a shaman, MPD, the Glass Delusion) throughout history not grounded in material reality. Everyone has rights to become their happiest self. The issue regarding the wording of this section is if others around them MUST adopt their self-perception as literally true. A more critical approach is warranted.
Some context: Gender Health Query is bringing this up due to our perspective as a medical & cultural watchdog organization around pediatric medical transition & contemporary gender ideology. We formed because we are starting to observe real-world harm to young people resulting from the gender identity movement despite its positives. This section assumes that genderfluidity ideology discourse is progressive & the healthiest possible framing for people struggling with gender issues. & that if we all believe that gender is indeed a spectrum, that there are multiple genders, & that this should be validated by not only health professionals but the public at large, that dysphoric people will experience reduced problems with mental health.
Many of us (we are an LGBT organization & trans-inclusive) have come not to believe that, & we have evidence. We range from LGB people observing body hatred issues in gender nonconforming young females not alleviated by transition to “transmedicalists” who believe that the genderqueer movement, with its myriad of pronouns & demands on the outside world for validation, is harming transsexuals (a term they embrace to distinguish themselves as having a definable medical condition).
The language you are using in this whole section is concerning because demands are being made. Demands that psychologists not only support their clients with kindness, compassion, & coping skills but must also adopt their clients’ worldviews & subjective experience as facts about gender (217-219). & this from the APA’s Nonbinary Fact Sheet:
“Practice using singular pronouns such as they/them & zie/ hir. Using non-binary pronouns can feel awkward at first. Practicing using these pronouns outside of the therapy room will allow clinicians to get more comfortable & fluent in doing so & will make speaking with clients easier.”
Not all LGBT people support the language used here because of where it has led. We are seeing some harm arising from telling young people that biological sex is irrelevant & that gender is a spectrum. “Harm” meaning a glorification of body dysmorphia now viewed as “cool” identities. Harm meaning an increase in stories of transition regret. Harm meaning “queer” youth who seem to have difficulty coping with even minor challenges to their worldviews about their long growing lists of sexual & gender identities & demands to be sexually & emotionally validated by people who don’t agree with identity over biology. Harm meaning any young bisexual who doesn’t want to identify as “pansexual,” or lesbian who doesn’t want sex with MtFs, is being called a bigot, an unhealthy form of sexual harassment disguised as social justice, behavior now rife in LGBT youth & even some adult spaces. Harm meaning young people who are so gender/sexually confused they are being put at risk for sexual exploitation by peers & adults online & in real life in “queer” spaces. Harm meaning an obsession with identity in youth culture over accomplishment & human values. We have many examples to justify these statements (see genderhq.org).
Guideline 2. Psychologists understand that gender identity & sexual orientation are distinct but
Mental health professionals should educate themselves on the specific & often-ignored needs of trans people & that trans & sexual orientation are two different things.
It is also important to acknowledge the association of even intense childhood dysphoria & adult GL identity (https://www.genderhq.org/trans-children-gender-dysphoria-desistance-gay/#anchor-page1-section-b). Evidence such as “the older brother effect” indicates certain biological processes create both trans & gay outcomes. Hormone in utero effects may affect FtM or lesbian identity (https://www.genderhq.org/trans-nature-vs-nurture-innate-gender-identity-culture). This is why there is a growing community of LGB people who are very concerned about socially reinforcing a child’s cross-sex identification at age 5 & giving them Lupron as early as age 11. & the push to socially & medically transition the large increase in trans-identified bio females. We don’t know the number of medicalized false positives that will occur, but it won’t be zero. There is currently a detrans subreddit (https://www.reddit.com/r/detrans/) with thousands of people in it & most appear to be L & B young women dealing with medical side effects who transitioned at too young an age.
In line 279, you use the term “Sexual orientation identity.” Sexual orientation is based on bio sex, as in male & female. It is not an “identity.” Individuals are free to view themselves as they wish. But our org. protests any attempt by mental health bodies to define gay & lesbian people based on gender identity & not same-sex attraction. We aren’t alone in this. If the APA adopts the stance that sexual orientation is something one can identify into, you are taking sides on an issue that is extremely contentious. You will be taking a position many gay men & lesbians view as offensive to the interests of their minority groups. Why? The answer is in the way this ideology plays out in the real world. Contemporary gender identity activism (that uses the same language used in this document) is framing gays & lesbians as bigoted for not including dysphoric, opposite-sex people in their sexuality. It’s causing much strife. There are even psychologists who are “problematizing” homosexuality & heterosexuality by framing not emotionally & sexually validating trans people’s identities in terms of social justice (Blair 2018). Our board had to write a response. https://www.genderhq.org/blog/2019/6/17/ghq-board-opinion-sexuality-as-social-justice-creates-problems-especially-among-lgbt-youth?rq=Blair
Some people in the LGB population will view the APA as a hostile entity to LGB identity if you validate the concept one can identify into homosexuality or gay & lesbian identity or that bisexuality is anything other than attraction to the 2 biological sexes. Changing these definitions reflects genderqueer activism, not facts.
Line 266 “range of gender identities that exist.”
The APA may want to consider if adopting queer theory views of gender as a spectrum is helping in the real world as it relates to NB-identified people. Most research showing benefits of transition relates to binary FtM & MtF. While studies such as Russel (2018) show a boost in happiness if pronouns are respected, & this may include third gender pronouns, other studies indicate many people are not being helped by the rise in the NB identity. Several studies on NB identities show they have worse mental health than binary trans people (Jellestad 2018, James 2016, Tebbe 2016). This is often blamed on the outside world’s failure to validate them properly. Our position is that youth should not be encouraged to seek & demand validation from others to achieve happiness, but the current genderqueer movement relies heavily on this concept.
Other plausible scenarios are persons may adopt an NB identity due to ASD, BPD, BDD, HPD, NPD, or AGP. They may be struggling with internalized anti-gay/lesbian feelings. There are personal accounts that say so & at least one study that shows homophobic bullying increases the likelihood of trans identification (Delay 2017). They may be experiencing a female inferiority complex as one of the many females identifying as trans or NB in exploding numbers. The compassion in this section is good. We want support for GNC people too. We must create space in society for them & support them. We ARE them as an LGBT organization. But mental health is complex & mental health issues should not be rebranded as “identities” because we believe that is what we see in some cases. Given affirmative model advocates openly admit minors are undergoing permanent medical alteration like double mastectomy for NB identities, the APA must look at what is causing this increase in mostly female minors with these identities. We are seeing more stories of transition regret & some of these mostly lesbian & bisexual or ASD young women had adopted NB identities.
Guideline 5. Psychologists recognize how stigma, prejudice, discrimination, & violence affect the health & well-being of TGNC people.
“Discrimination can include…not using a person’s preferred name or pronoun”
We hope the APA believes there are limits to defining not using preferred pronouns as “discrimination” given there are now dozens of them. Is an LGB person or transmedicalist “discriminating” against someone if they do not believe in pronouns such as ze, ve, zir, they, & it, all pronouns you will see people use. The APA must be mindful not to advocate for imposing worldviews on others who may not agree with them by framing it as bigotry & discrimination. This is an increasing problem in academia & has infiltrated science bodies. Real discrimination is kicking someone out of a home or firing them.
Discrimination, suicide ideation, mental health issues, & violence inflicted on poor black & brown people are all real issues that must be addressed. We also see a huge amount of paranoia in the trans community that is not in line with reality when one examines crime statistics. Trans people overall may not be at higher risk for violence relative to other groups such as women in general or black men. & the media reported murders, with hyped headlines, often involve situations where they weren’t targeted in an anti-trans hate crime. One study shows they are at lower risk for violence than women overall. Since anxiety, depression, suicide ideation, & paranoia are all socially contagious phenomena, it is best to educate trans people about how to be mindful to keep themselves safe & healthy without fomenting fear that may harm their mental health and make them feel hated. Targeted programs for poor people at risk for drug addiction & prostitution are most needed. Trans people can live safe & happy lives in tolerant areas. It is crucial to promote messages of hope.
https://www.channel4.com/news/factcheck/factcheck-how-many-trans-people-murdered-uk
https://quillette.com/2019/12/07/are-we-in-the-midst-of-a-transgender-murder-epidemic/
https://www.washingtontimes.com/news/2019/dec/8/transgender-homicide-rate-remarkably-low-despite-h/
This section mentions “stigma.” Our position is that many mental health professionals are participating in stigmatizing autogynephilia by refusing to recognize it exists due to political pressure from certain activists. Many trans people admit they experience this. We believe we see a lot of harm, shame, & acting out resulting from people participating in AGP denial.
https://www.genderhq.org/trans-youth-identity-politics-rights-conflicts-lgbt-part3
The APA should start talking about this condition openly. We consider it malpractice to continue to deny it exists, which may prevent a therapist from helping people in the most honest way possible without shame.
Guideline 7: Psychologists understand the need to promote social change that reduces the negative effects of stigma on the health & well-being of TGNC people.
Some concerning parts of this section-
"Psychologists may choose to become involved with an organization that seeks to revise law & public policy"
"Psychologists may consult the National Center for Transgender Equality"
This is an ideological trans rights organization. For example, they make these claims about trans students- "Some are denied opportunities to go on field trips or participate in sports."
This is a lie. People want policies to protect female students & female sports. All evidence is leading to MtFs having very significant biological advantages in sports over biological females even once they medically transition (https://fairplayforwomen.com/sports/). MtFs are blowing away females in track in high school and college, for example. No one is preventing anyone from participating in sports based on biological sex. FtMs on testosterone may be included in male sports if they wish as they will still retain a disadvantage but have unacceptable advantages over girls and women. We believe males need to learn to be kind & compassionate towards gender nonconforming males who may identify as girls, not force girls to be nurturers at the expense of their ability to win sports competitions because they don't matter as much as a male with GD. There is a trans Muay Thai fighter who identifies as a trans woman & fights males and recognizes they are trans & takes pride it that. This is preferable role-modeling, not forcing society to deny biological reality.
Imagine an unaltered MtF goes on a field trip, stays in sleeping quarters with a girl & has consensual sex with her on a school field trip. She gets pregnant. That is a situation where the parents will have every right to sue the school. A school worried about this is not "discriminating" against a trans student who is undoubtedly allowed to attend field trips as any other student. Safe, compassionate accommodations must be made for all. The APA should not follow organizations such as this uncritically for advice.
The APA should stay away from inserting itself "to promote social change" when it results in potentially harming other groups. Adhere to "change" that protects the safety, health, & ability to live & work for trans people. If you go beyond that & promote current gender identity activist demands like MtFs are "literally female," you will be viewed as an anti-woman & anti-LGB rights organization by many. The eradication of women's sports, prisons, rape crises centers for biological females, medicalizing children who may be pre-LGB, & eliminating the ability to collect valid data regarding sex due to the change of public records are very contentious issues. Many people, including conservatives, far leftists, trans-rationalists, LGB people, parents, feminists, scientists, and detransitioners are working against some of the biology denialism in current gender identity activism. LGB people are breaking off from LGBT organizations to form new ones due to this ideological capture. Best avoid "promoting social change" in those areas unless you want your organization torn apart by this.
Guideline 8. Psychologists working with gender-questioning 4 and TGNC youth understand the different developmental needs of children and adolescents, and that not all youth will persist in a TGNC identity into adulthood.
"As a result, this research runs a strong risk of inflating estimates of the number of youths who do not persist with a TGNC identity."
This is debatable when one takes a close look at the Steensma study.
https://medium.com/@jesse.singal/everyone-myself-included-has-been-misreading-the-single-biggest-study-on-childhood-gender-8b6b3d82dcf3
We review desistance stats here.
https://www.genderhq.org/trans-children-gender-dysphoria-desistance-gay
We already know false positives on minors are happening. We just don't know the numbers. The APA should take this on as an ethical duty. Detransitioners will be a growing population. We see rapid validation of trans identity in minors by psychologists leading to irreversible medical consequences. At the same time, we see young people who meet full DSM criteria but are desisting or detransitioning. These are minors being put under extreme medical protocols. It's good always to be mindful of this reality. Transition underage is considered a human right now. Is growing up without being permanently medically altered for intense, but ultimately transient feelings a human right? We believe it is.
We consider stories like this malpractice. This 15-yr-old girl would have taken testosterone had her father not let her before desisting after meeting DSM criteria. As a medical watchdog org, we hear a lot of stories like this. Altering physically healthy bodies underage would normally be considered a major human rights violation. The inevitable false positives on mostly pre-LGB youth, ASD, and girls with trauma that will result from transitioning youth before brain maturation are acceptable collateral damage to trans-positive healthcare. This is the reality of the new paradigm, and we would like to see organizations like the APA be more upfront about it, given the serious medical consequences. For example, altering pre-LGB youth can be considered akin to what was done to intersex babies when doctors surgically altered them given the Lupron to estrogen protocol stunts genital growth, and they are doing surgeries underage now.
https://www.genderhq.org/blog/2020/4/8/teen-girl-outgrows-gender-dysphoria-dangers-pediatric-medical-transition
Medical transition under age causes sterility, may permanently destroy sexual function and may impact cognition and bone health.
https://www.genderhq.org/trans-youth-side-effects-hormone-blockers-surgery
"Much greater consensus exists regarding practice with adolescents. Adolescents presenting with gender identity concerns bring their own set of unique challenges."
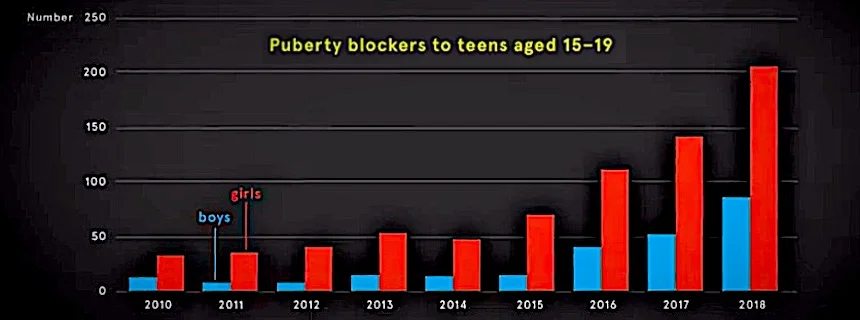
This comment should be removed. The demographics of this condition have completely changed, with many more females seeking SRS, more heterosexual females wanting to be gay men, and an overall increase in youth requesting medical treatments. There is not a consensus about what to do. The Tavistock gender clinic in the UK has seen multiple public resignations. That doesn't indicate "consensus." It indicates safeguarding and ethics problems. It's unethical as a mental health body to not to take a closer look at ROGD and other trends when one sees these graphs. We believe there is very robust evidence GD is a socially contagious and iatrogenic condition for some people, particularly female teens and YAs.
https://www.genderhq.org/increase-trans-females-nonbinary-dysphoria
Much evidence points to social factors contributing to GD. Society is currently being set up to maximize the number of medicalized young people.
https://www.genderhq.org/trans-nature-vs-nurture-innate-gender-identity-culture/#anchor-page10-section-a
Guideline 11. Psychologists recognize that TGNC people are more likely to experience positive life outcomes when they receive social support or trans-affirmative care.
We have reason to believe younger cohorts will have more regret and less positive mental health outcomes due to the substantial increases in the numbers of young people transitioning and the move to the affirmative model and informed consent model for adults. For example, the Williams Institute study is touted as an example of a study validating the need to offer easy medical transition access. But if one looks at the question about passing better, there is no benefit. In that study, natal females (in contrast to natal males) who say other people don't recognize them as trans or GNC have the same or higher suicide attempt rate as females who are dysphoric and recognized as female, not male.
If you look at Lipson (2019) there are incredibly high rates of mental health problems among the trans college students surveyed. This is at a time when celebration of trans identity is at an all-time high. And college students are often given access to transition healthcare. Yet the rate of mental health problems is alarming, particularly among biological females. Given it is known females are prone to body dysmorphia contagions or BPD, which involves identity instability, we hope the APA is asking questions beyond blind affirmation. We are seeing many therapists blindly and immediately affirming young people assuming transition will solve all of their problems. It's one reason we felt we had to form GHQ.
Another recent study (Branstrom 2019) calls into question the overall benefits of SRS on mental health. The conclusions of this study initially claimed a benefit. The study had to be corrected after several LTEs pointed out major flaws. It showed no benefit. It's disingenuous they have not changed the title, and bias may be involved in them not retracting it altogether.
https://ajp.psychiatryonline.org/doi/abs/10.1176/appi.ajp.2019.19010080?journalCode=ajp
https://www.genderhq.org/blog/2020/8/19/american-journal-of-psychiatry-study-purported-to-show-benefits-of-transgender-medical-transition-made-false-claims
We review the positive studies on GHQ.
https://www.genderhq.org/trans-youth-suicide-statistics-kill-themselves-manipulate-parents/#anchor-page15-section-b-what
We also cover studies such as Dhejne, Adams, and Marshall that call into question the positive effects of medical transition in the long run on mental health & suicide risk.
https://www.genderhq.org/trans-youth-suicide-statistics-kill-themselves-manipulate-parents/#anchor-page15-section-b-below
The APA may want to take a closer look at what is going on now rather than rely on the Cornell review and other positive studies. Detransition and rapid onset gender dysphoria (Littman 2018) will likely be growing topics. Please don't acquiesce to the intense and often successful efforts to shut this down.
https://www.reddit.com/r/detrans/
https://www.genderhq.org/trans-activism-identity-politics-harassment-censorship
Guideline 15. Psychologists respect the welfare and rights of TGNC participants in research and strive to represent results accurately and avoid misuse or misrepresentation of findings.
“One group of experts has recommended that population research, & especially government-sponsored surveillance research, use a two-step method, first asking for sex assigned at birth, & then following with a question about gender identity (GenIUSS, 2013).”
Yes- it is critical to collect data knowing the biological sex of all involved. This is creating problems. We look at studies on LGBT youth and we don’t even know the biological sex of those involved. It’s an example of the many problems identity over biological reality causes. Scientists, women, gay people, and trans people all need access to proper data.
Thank you so much for allowing us to participate.