TOPICS
For those new to this issue it’s best to know these terms before reading.
11) Why are so many females coming out as trans/non-binary?
A. Evidence for large increases in females identifying as trans
While the explosion in referrals of children and adolescents to gender clinics could be explained by greater societal and parental awareness and children feeling more comfortable in expressing they have issues with their gender, what is more difficult to explain is the drastic sex ratio reversal of females presenting with gender dysphoria. Not all of them will necessarily medically transition, but more and more females are distressed enough about their gender to seek mental health and medical advice. It is important to understand what is driving this trend.
It is relevant to note that while more people may be claiming trangender identities, the current observed ratio of females to males with gender dysphoria in youth clinics does not match the numbers of transitioners in the adult population in the recent past. Most of the earliest gender transitions were MtF in most countries. According to the authors of this study:
In adult samples [of transitioners], in almost all cases, the number of natal males either exceeds the number of natal females or the sex ratio is near parity.
The ratio has balanced out recently and in many western countries, with the ratio favouring females.
One hypothesis for this increase in referrals is chemicals in the environment, such as in drinking water which mimic hormones. However, it is an unlikely explanation because they are mostly estrogen mimicking. This would lead to an increase in males with gender dysphoria, not females. Also, these hormone mimicking chemicals cause females to go into puberty earlier. Early hormonal puberty has been not been ruled out as a cause, but research has found not connection with GD and early puberty in girls (Aitken et al).
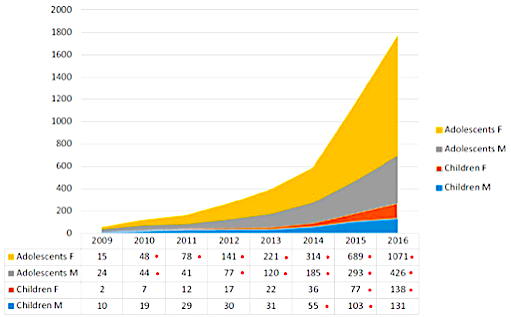
This chart from TransgenderTrend shows the sex ratio over time in those presenting to the Tavistock gender. This trend is representative of the observed trend throughout the Western world.

The Tavistock clinic shows significant increases of gender dysphoric minors presenting to gender clinics for gender-related distress over time.
This chart, Kaiser Permantente (U.S.) illustrates the growing trend and offers a look at a cross sectional population study, broken down by age.

Chart compiled by a 3rd party from a population of Kaiser Permanente patients
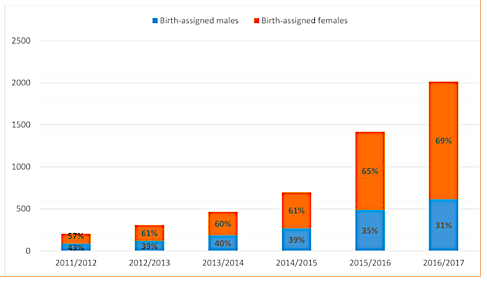
The below graph shows the increases of trans-identified females in New Zealand (all ages):

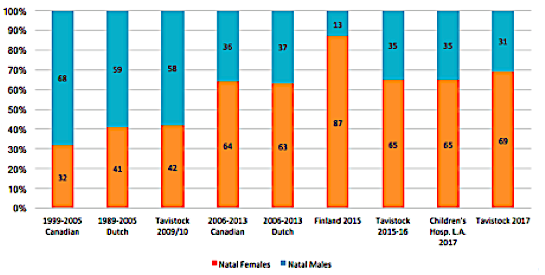
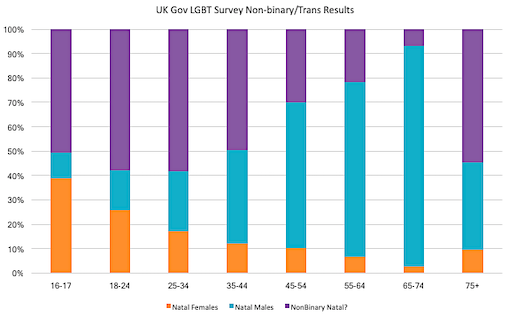
The below chart demonstrates that this trend towards a large increase of natal females is happening in Western countries in general.
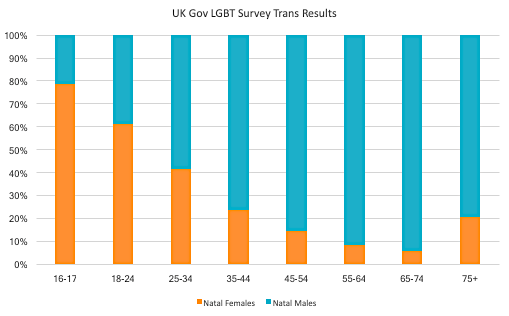
This is a chart compiled from a 2018 online trans survey conducted by the UK government. Voluntary surveys are not the most accurate way to obtain information. However, the sex ratio reversal in this survey is consistent with referrals to other gender clinics. The over age 75 outlier may be due to the fact that biological females are outliving biological males in that age cohort.
genderhq
In some studies (see below) at least 2/3 of those identifying as non-binary are females. If we make that assumption for the UK survey, the numbers of females who reject their womanhood is even larger relative to males.
genderhq
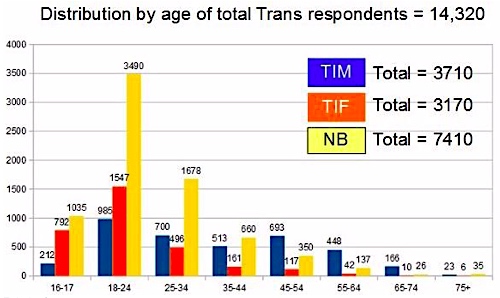
Here is a graph of the same data by Fairplayforwomen.com:
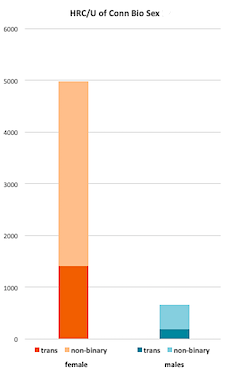
A recent survey study (mean age 15.5 yrs) done by the HRC and the University of Connecticut highlights the large number of females who identify as “trans boys.” The study failed to verify biological sex which demonstrates one of the problems that arise when scientific research becomes affected by postmodern gender theory. However, it is reasonable to assume that “trans boys” are biological females. It is also important to note that they also failed to verify the biological sex of non-binary identified youth.
Survey studies, by their nature, have flaws. It should be noted that this is not a population based study. Results were acquired online and likely more representative of online “queer/LGBT” spaces. What is illuminating, however, is that female outnumber male. The ratio of “trans boys” to “trans girls” in this survey is over 7.5:1.

Here is a link to more detailed findings in the study (Watson et al. 2019) and a table breaking down the numbers across various categories:

If non-binary identities are considered as well as binary trans identities, this ratio becomes even greater. See the graph below for the breakdown of trans identification by biological sex:
(4977 female : 660 male)
Another interesting finding of this survey is, that unlike the pattern of same-sex attracted youth seeking medical transition (mostly homosexual) found in previous studies, there is a very large percent of “bi/pan/queer” females adopting trans identities (ftm and “transmasc”). This is also true of females who identify as “gay boys.” This indicates changing demographics in not only numbers, also sexual orientation cohorts. Aitken et al and Littman 2018 confirm this as well.

genderhq from HRC U of Conn LGBT survey 2018
Surgery for FtM identified females has increased by 289% in just one year, according to this Plasticsurgery.org data.


Affirmative model advocates’ explanations for increasing numbers of trans identified females
There are a number of arguments as to why there is recent rapid rise in females seeking treatment for gender dysphoria in puberty or post puberty, and why their numbers are higher than those for natal young males. While they may have some validity, these arguments or explanations are only speculative.
1) Age of onset gender dysphoria happens later for females than males.
Olson-Kennedy speculates that genital dysphoria may be more common in young trans girls because a penis is such a central part of what society associates with being a man.
Females, then, become dysphoric when they start to grow breasts because that is what is associated with womanhood.
Response: While this may be true, this explanation does not fully explain why the presence of a penis would create more distress in a dysphoric male than the lack of a penis in a dysphoric female. If the female’s innate gender identity is male, why would the lack of a penis, with it’s “societal” importance of a penis (Olson-Kennedy points out) to male identity, not be distressing?
2) Feminine behavior in boys is more stigmatized so parents are more likely to bring in effeminate males to be assessed than tomboyish females.
Response: This is likely a correct explanation as to why there were more prepubescent feminine males brought to clinics previously. It does not explain why more females are coming to gender clinics than males in a ratio that is far higher than in recent adult populations studies. More young females are asking to go to these clinics regardless of the behavior of the parents. Why?
It may be that gender non-conforming females, who are more likely to grow up to be lesbians, are more likely to be accepted as trans by their parents. For example, parents appear more enthusiastic about medically transitioning butch daughters than effeminate sons. Below is a quote reviewed in a previous topic around the fact some parents may prefer a trans child to a gay or lesbian one.
Johanna Olson-Kennedy when talking about having to go to court if parents weren’t on board with a transition says:
“By the way, I have never had to do this with a trans boy. It’s always trans girls.”
This study of Californians also supports the observation that parents are quicker to adopt the view their child is, in fact, transgender if they are masculine females.
This may not be surprising in light of the fact that doctors are apparently willing to administer potentially dangerous drugs to mothers to prevent an increased likelihood of having a lesbian (or even just tomboyish) daughter, “The Anti-Lesbian Drug.”
3) It’s just more accepted for females to transition and there is less social cost for being FtM.
This is argued in Aitken et al:
Thus, it could be argued that it is easier for adolescent females to “come out” as transgendered than it is for adolescent males to come out as transgendered because masculine behavior is subject to less social sanction than feminine behavior. Some support for this was found in Shiffman’s [31] study of peer relations in adolescents with GD, in which adolescent males with GD reported more “social bullying” than adolescent females with GD.
Response: It may be accurate to say FtMs have less social costs to transitioning in some ways (ex. FtMs have their wages go up post transition). However, this would have been just as much a reality ten years ago as it is today and perhaps even more so and should also be reflected in the adult population.
The reverse argument which is just as plausible is neglected by affirmative model advocates. Butch lesbians and other masculine or even androgynous females are not valued in society and this contributes to their body dysmorphia. The increase of attention on trans issues has acted like an advertisement program for cosmetic surgery as a solution to this problem.
4) Another argument is that natal males are bullied more for being effeminate than masculine females, which may influence them not to seek transition. Again, this is argued in Aitken.
Response: In reality the bullying could have the opposite effect. Feminine boys would want to go through with transition to fit gender norms rather than be discouraged from transitioning because of their femininity. This study on homophobic bullying influencing trans identification indicates exactly that. The study, as well as other examples found here and below, also don’t indicate masculine and/or lesbian girls are less ostracized than effeminate boys. If masculine, androgynous girls are are more accepted, we would expect less biological females presenting to gender clinics, not more.
5) Another hypothesis is that there have always been more transmen and past studies have not captured this:
“When you look at the earlier studies [of the make-up of adult trans populations], what you see is that they’re collecting data on genital surgery,” Olson-Kennedy explained. “But the reality is that it’s easier to surgically create a vagina than it is a penis—there’s just no way of knowing how many trans men there always were that studies missed.”
Response: This argument does not make sense based on genital surgery, but mastectomies which are easier to perform and much less risky than vaginoplasties have only recently increased in rates.
6) Youth gender dysphoria ratios are likely to look different than adult ratios and will even out over time. Homosexual transsexuals (natal males attracted to men) come out earlier than MtFs who are attracted to women. “Late onset” (autogynephilic) MtFs generally come out in later adulthood, rather than present as extremely feminine and dysphoric as children, as homosexual transsexuals do. Perhaps biological males will come out later.
Response: A large percentage of MtFs who transitioned in the past are/were autogynephilic heterosexual males. Not all, but the vast majority of FtMs in the past who transitioned were homosexual females who did at times transition in adulthood, rather than as adolescents. While these females may just be coming out younger, this doesn’t explain why the increase in social tolerance is not causing heterosexual MtFs to come out in such large numbers as well, especially since they used to be the majority of those seeking medical transition
This argument is explored further on the blog Thehomoarchy.com:
I thought there may be a reasonable explanation for this extreme sex ratio reversal in such a short period of time. Trans people are diverse but there are different types of MtF trans people. One type is very effeminate as young children and are almost exclusively attracted to males. The other general type is considered “late onset” as they tend to come out later and are generally attracted to women or are bisexual or asexual. I assume the late onset type, who actually make up a large percent of the trans community, may be under represented in the tween/teenage groups. But that’s not the case in these studies. They are coming out at younger ages as well.
‘1976-2005 – 67% primarily attracted to males, 33% other
1) 2006-2013 – 44% primarily attracted to males, 56% other- Transresearchinfo.com
-There is a significant increase of females with a bisexual or heterosexual attraction with regards to their natal sex seeking treatment for gender dysphoria. The Canadian clinic looked at the sexual orientation of the young people. The known epidemiology of this condition has shifted rapidly. The topic of youth transitions is becoming more relevant for the bisexual community and not just gays and lesbians.1) 1976-2005 – 89% primarily attracted to females; 11% other
2) 2006-2013 – 64% primarily attracted to females; 36% other- Transresearchinfo.com
A quote from the same blog post can be a response that applies generally to what looks like a desire to confirm positive reasons for increasing numbers of females seeking breast amputation and hormones for trans and non-binary identities. There appears to be motivations to not explore possible negative explanations among affirmative model advocates or even more cautious researchers. Even if the positive explanations turn out to be true, it is the role of psychologists and doctors, who are facilitating permanently altering and potentially sterilizing treatment on minors and young adults, consider all possibilities.
I would argue it was negligent on the part of the authors of this study to not even consider this shift in the context of the fact that females experience significantly more body hatred than males. This manifests itself in more cutting, dieting, anorexia, bulimia, and plastic surgery. Labiaplasty is now becoming more popular among teenagers and young women, so their genitals can conform to porn star representations. All of these behaviors in females were at one time nonexistent or rare but became popularized through social contagion due to increased media attention. I’m not saying anorexia in the same as gender dysphoria. There are similarities and there are major differences. Sex reassignment surgery can relieve symptoms and aid in health and purging always worsens it. I am only arguing that it is unprofessional and a sign of self-protection on the part of these authors not to even bring up the issue of female body shame. And the reason they avoid this basic “Sociology 101” question in my opinion, is because it would force these researchers to consider they may be playing a part in increasing the very thing they are trying to treat.
Information indicating all may not be well with trans identified females is in fact being censored by media, the mental health profession, and public universities. The Dean of the public health department at Brown University supported removing links (in an effort to limit public access to this information) to the below peer-reviewed study for failing to provide a completely positive narrative around trans identified youth as expressed in this study :
There were 256 parent-completed surveys that met study criteria. The adolescent and young adult (AYA) children described were predominantly female sex at birth (82.8%) with a mean age of 16.4 years. Forty-one percent of the AYAs had expressed a non-heterosexual sexual orientation before identifying as transgender. Many (62.5%) of the AYAs had been diagnosed with at least one mental health disorder or neurodevelopmental disability prior to the onset of their gender dysphoria (range of the number of pre-existing diagnoses 0–7). In 36.8% of the friendship groups described, the majority of the members became transgender-identified. The most likely outcomes were that AYA mental well-being and parent-child relationships became worse since AYAs “came out”. AYAs expressed a range of behaviors that included: expressing distrust of non-transgender people (22.7%); stopping spending time with non-transgender friends (25.0%); trying to isolate themselves from their families (49.4%), and only trusting information about gender dysphoria from transgender sources (46.6%)…
Parents have described clusters of gender dysphoria outbreaks occurring in pre-existing friend groups with multiple or even all members of a friend group becoming gender dysphoric and transgender-identified in a pattern that seems statistically unlikely based on previous research [1–5].
In Britain, enough individuals are concerned as to warrant a government inquiry into the increasing numbers of trans identified females. The sections below cover some material as to why this inquiry is a good idea.
B. Females experience higher rates of body hatred, certain types of self-harming, and anxiety/depression that may influence a trans identification

Self-harm stats in UK, graph Secondary Care Analysis, NHS Digital,

GIDS UK. Is GD related to increase of self-harm in females
Transition to treat gender dysphoria may reduce self-harming behavior and improve body image as shown in these studies. But with the changing demographics of gender dysphoria it is worth considering that cases are becoming more complicated and that there may be other issues going on with young females that may not be solved by transition.
While males and females experience similar rates of body dysmorphic disorder, overall it is well-established that women/girls are more prone to issues of body dissatisfaction or even outright body hatred than males.
Women are up to ten times more likely to have a poor body image than men.
Depression and anxiety are also higher in females than males and are often comorbid with body dysmorphic disorder.
Despite the avoidance of this topic in pro-affirmative model conferences held by organizations such as Gender Odyssey and WPATH, the British clinicians at Tavistock have considered the possibility that some of these cases may be more similar to other female body dysmorphias, rather than these females expressing their “innate” gender. The Tavistock clinic now has a 3:1 female to male ratio with many presenting serious comorbid conditions. Dr. Wren (audio linked now removed) explores the reality that many females hate their bodies in a cultural context. It is a subject that psychologists should explore in the interests of due diligence.
It could be argued that we live in a society where there is a disproportionate emphasis on physical appearance and huge pressure to attain an ideal body type. In this context it may be disproportionately young women who hate their bodies if they feel that cannot attain these ideals, and who wish to act on their bodies in some way, for example through restrictive dieting and body modification. However, it would be speculative and simplistic – and from our point of view premature – to suggest that this is the main reason for the increase in referrals of natal females to our service.
Eating disorders (anorexia, bulimia, unhealthy dieting practices) are much more common in females than males. It is difficult to know how much of this is nature and how much is nurture. It appears to be a combination of both. There appears to be brain activity differences that explain some of this:
Interestingly, researchers found that during the experiment, a direct link was observed between parietal lobes, the area of the brain connected with body perception, and the area of the brain associated with the processing of subjective emotions, such as anger or fear. Women participating in this study demonstrated more prominent brain activity in response to “owning” a body that is obese compared to their male counterparts. These findings led researchers to conclude that higher body dissatisfaction in women is experienced for these neurobiological reasons.
This study focuses on the intense cultural pressure on women to be skinny and beautiful.
Evidence for the more intensive pressure on women to be slim is presented. Other contributory factors that serve to intensify women's struggle to control their weight and shape, such as adolescent turmoil, poor body concept, and role confusion, are also reviewed.
While males do participate in self harming behavior through substance abuse and violence, females appear to turn this more inwardly on themselves. This Vice article discusses the current rates of self-harming in Britain. It’s increasing and higher among girls. This article relates it to other historical examples of self-harming behavior. This study also states that this body dissatisfaction in girls begins as young as three years old.
Self-harm among teenagers is pretty close to an epidemic in the UK. Evidence about the exact number of self-harm cases is scattered, but almost every report published in recent years has shown that it's on the rise. In 2014, figures were published showing a 70 percent increase in 10- to 14-year-olds attending A&E for self-harm—related reasons over the preceding two years. Last year, a wide-reaching survey conducted by leading civil servants found that a third of 15-year-old girls had reported harming themselves on purpose. Earlier this month, a report from ChildLine found the charity is now mostly receiving calls about low self-esteem, bullying and self-harm. In 1986, when the 24-hour helpline began, children's top concerns were sexual abuse, family problems, physical abuse and pregnancy—calls about self-harm were not recorded at all.
Forbes referencing the same study:
Nearly three in four of these youth (73%) were girls, and the remaining 27% were boys. Unsurprisingly, more than a third of these girls and over a quarter of the boys had been diagnosed with a depression or anxiety disorder.
Girls were also more likely to have an eating disorder, but boys were more likely to have a diagnosis of attention deficit hyperactivity disorder, autism spectrum disorder, conduct disorder or a type of schizophrenia disorder.
This problem is getting so bad, the school systems in Britain are having trouble coping with all of the self-harming cases.
Schools are struggling to cope with a surge in self-harm among children, with more than 70,000 incidents in secondaries last year, research by The Times suggests.
The number of incidents recorded by schools has more than doubled since 2012, according to figures obtained through freedom of information requests.
School nurses are dealing with panic attacks, self-cutting, overdoses and eating disorders rather than the nose bleeds and minor accidents of a decade ago. Head teachers voiced frustration at a lack of mental health support…
Low-level harm, including friction sores known as “chicken scratches”, was treated less seriously by some schools. Copying peers and emotional contagions, when taken together, were the cause most frequently logged by schools. Family problems, social media, bullying and problems at school were also common factors. Girls were far more likely to harm themselves than boys were, although teenage boys were more likely to take their own lives.
Here is a chart containing some of the UK’s study’s findings:

UK information is helpful in understanding patterns of gender dysphoria and other mental health problems due to their public health system. These increases of self-harming , which is also more prevalent among girls, can also be found in the United States.
Self-harm or self-injury, the act of hurting oneself on purpose, affects nearly 1 in 4 teenage girls in the United States...
Still, more than 1 in 10 high school boys in the analyses reported NSSI.
Given the changing demographics of females with gender dysphoria, newer sexual orientation such as pan gender, and new gender identities in which females identify more as non-binary than male, it’s reasonable to ask if some of these aren’t cases of body dysmorphic disorder. Chest binding, something that can cause dizziness due to shortness of breath and cracked ribs used to be rare even among same-sex attracted females who made up most of the population that started transitioning in higher numbers in the 1990s. But now, so many female teenagers are binding that schools are having to implement binding policies. Some advice given to schools in Britain:
“hot, uncomfortable and restrictive – but very important to [pupils’] psychological well being”. Teachers are nonetheless told to remain aware of the risk of “breathing difficulties, skeletal problems and fainting.”
Dr. Norman Spack, a pro-early social and medical transition advocate, displays some level of ignorance about the intensity of fear, awkwardness, and shame many females have about their bodies during the onset of puberty in particular. This includes the beginnings of body dysmorphic disorder.
The difference between a tomboy and a trans-male who starts puberty, is that the tomboy accepts having breasts and having periods.
Jack Monroe, who vacillates between identifying as non-binary and still identifying as a woman, has had a double mastectomy because of breast disgust and wanting a more androgynous appearance. She provides the opportunity to examine a particular case of breast amputation for a non-binary identity.
Thousands upon thousands of women have breast enhancement surgery every year to alter the “natural” configuration of their chests to match how they would prefer it to look. One of my cousins underwent a breast enlargement a few years ago, and her family and friends were supportive, accepting her explanation that the procedure would increase her self-confidence. Yet when I announced that I wanted a chest reduction, I was met with horror and stony silence from certain members of my family. “You can’t.” Well, yes, I can.
While this is an interesting point about a family’s supportive attitude towards artificial breasts, it is not the best comparison to argue that cosmetic surgery improves mental health. Jack Monroe, who has stated herself she has had a myriad of mental health issues, including gender dysphoria, a “severe eating disorder,” and anxiety and depression, fails to mention that breast enhancement does not seem to address the psychological issues underlying the body dysmorphia. Hopefully, Jack Monroe will remain happier post-surgery but it is now known that women who get breast augmentation have higher rates of suicide than the general population.
Women have an overall threefold higher risk of suicide after getting breast implants -- a risk that keeps going up over time, a new study shows.
Loren Lipworth, ScD, Joseph K. McLaughlin, PhD, and colleagues analyzed data on 3,527 Swedish women. The women had voluntary cosmetic silicone breast-implant surgery an average of 19 years earlier.
"It appeared there was no excess risk of suicide in the first ten years after receiving a breast implant," Lipworth tells WebMD. "But after that, the risk went up and continued to go up. There was a 4.5-fold risk for ten years after surgery and a sixfold risk for 20 or more years."
The women also had a threefold higher risk of alcohol or drug dependence and an excess of drug/alcohol-related deaths from accident or injury.
Also, BDD is more common in women who seek breast implants in the first place.
RESULTS: Body dysmorphic disorder was significantly more prevalent in breast reconstruction patients than in the general population (17% vs 2%; P < .001). It also was much more common among patients who planned to undergo delayed (vs immediate) reconstruction (34% vs 13%; P = .004).
CONCLUSIONS: Relative to the general public, significantly more women who sought breast reconstruction were diagnosed as having BDD. Awareness of the potential for BDD will enable clinicians to better understand their patients' perspectives and discuss realistic expectations at the initial consultation. Future studies are warranted to examine the implications of BDD on patient satisfaction with reconstructive surgery.
Non-binary identities that require hormones and surgery have not been studied enough to know if they are true gender dysphoria or more like BDD. Surgeries do not solve the mental illness involved in body dysmorphia motivated cosmetic surgery, even if there is an initial honeymoon period. Michael Jackson is the most famous example.
There are young gender dysphoric females who have themselves stated trans identification overlaps with body dysmorphic disorder. This young woman who has a blog called, Destroy Your Binder, and struggles with gender dysphoria and body hatred herself, makes the connection between gender dysphoria and female body hatred:
What I believe now is binding is ultimately a form of self-harm.
Another young woman who identified has trans for several years as a teenager and desisted has this to say,
When I was first referred to the Gender Identity Service (GIDS), I was just a young girl who was confused, miserable, couldn’t fit in with her peers and was desperate to put a label on the awful feelings that plagued her. Every doctor I spoke to agreed whole-heartedly that I was transgender…My school was more than accepting; if anything, they were actually excited to have me. It started to feel like I was the beacon of diversity in my school…My transition moved along smoothly. I started hormone blockers (and got over my fear of needles) and there was some serious talk about getting referred for the surgery that would rid me of my cursed double-ds.
A year after I dropped out of school, a month after my eighteenth birthday, mere days before I was scheduled for the last hormone blocker before I moved onto testosterone, I realized what my problem was, I’d been misdiagnosed.
Lost in the honeymoon stage of having a name for the horrible sensation of feeling trapped in my body, I hadn’t even stopped to question it. I trekked on through the doubts, sure of myself and the diagnoses from so many doctors.
I tried to lie to myself. I started to feel like I was doing something wrong, like I was betraying myself, giving my whole identity up. I felt like I was sullying the good transgender name, like I was letting down everyone I’d met on my journey.
In the end, I realized there was nothing for it. I didn’t have gender dysphoria, I have body dysmorphia. I don’t have an issue with my gender, I have an issue with my self-image, brought on by my weight. Speaking to GIDS about it confirmed it.
Another detransitioner realized that transitioning was a form of self-harm for her:
I was passionately convinced I was transgender. A belief only augmented by the discovery of words like ‘non‐binary’ and ‘genderfluid’. Clinging to this new lexicon like my life depended on it; I thought I’d finally discovered my true identity and was hostile to all who suggested otherwise. Whilst I was busy shrouding myself in trans rhetoric, I continued to inject testosterone. I damaged my voice and I grew a lot of very dark, coarse hair on my face that I now have to epilate regularly. I have no idea if I am now infertile.
When I told my Dad what I was doing his rather unsympathetic response was ‘For God’s sake, is this just another form of self‐harm?’ At the time I raged at this blatant transphobia. I never thought I would admit he was right.
Though I only took testosterone for a year, I bound my breasts and wore only men’s clothes for considerably longer. I gave up binding six months ago and am cautiously exploring women’s clothes. Though I’m sure I’m not trans, overcoming my fear of femininity is an ongoing process.
I know now that my belief I was transgender was largely due to internalized misogyny and homophobia. Once I realized the truth, my dysphoria all but disappeared and I feel much happier in myself.
Dr. Wren expresses concern around female body hatred in a public discussion:
Could I just quickly respond to that? In many ways, we feel we are at the cutting edge of a huge social revolution—and it is a social revolution that many of us have really fought for and wanted around sex and gender and diversity and its acceptance in society—but where we are heading is really unknown to many of us. That is what we would talk about with Gendered Intelligence quite a bit, with these young people. For example—this is one group we did not mention—a much higher proportion of natal females is coming forward who have got through to puberty but who now really dislike their female body. I have to see that in the context of the attack on female bodies and the general sense that feminism has not delivered.
Research & historical evidence indicates females acquire mentally troubled feelings socially & more often than males.
Consider this discussion by an alarmed psychotherapist who left the gender transition profession:
Last week in a team meeting, our medical director said he was meeting with a girl who identifies as FtM to discuss top surgery and testosterone treatment. Apparently, according to the director, the girl’s mom is slowing down the process of transition. Bad mom, right? The director added that the girl’s mom told her that nine out of nine of her daughter’s friends also identify as FtM.
At this point I couldn’t hold my tongue any longer. I said, “Can we not be honest and see that we are dealing with a trend?” Of course, everyone else at the table was mute. Considering I’m leaving my post, I felt bold enough to say that I found it infuriating we couldn’t discuss this topic clinically. More silent colleagues (except their eyes were wide as if they wanted me to keep talking and taking the risk for them). I said that what we were doing as a medical community, was potentially very harmful, and made mention of some of the videos I’d watched featuring transmen who decided to go off testosterone. The medical director prides himself in providing special services for those patients he deems unjustly marginalized by society. But he can’t see how the medical community has become complicit in the oppression he earnestly seeks to remedy.
And this article which addresses previously unheard-of numbers of trans identified minors, mostly females:
A school which was hailed as the “coolest state secondary in town” has 40 children who do not identify with their gender.
Forty pupils at Dorothy Stringer High School - aged between 11 to 16 - do not identify with their gender assigned at birth while 36 said they are gender fluid…
On YouTube, testosterone is revered as “T”, “vitamin T” or “man-juice”. The side-effects are rarely mentioned. Vloggers urge you to “just do it . . . it’s all good”. There are tips for handling parents, claims that transition “saved me” from suicide and warnings that if you do not act quickly, you too could die.
“People are embarking on medical transitions they may not need or want in the end,” said Jane Galloway. “I fear greatly that in 10 to 15 years’ time, we will find ourselves with a slew of young adults with mutilated bodies, no sexual function, who will turn round to the NHS and ask, ‘Why did you let us do this?’ ”
Intriguingly, in every year for the past five, the NHS area covering Surrey, Kent and Sussex, which includes Brighton, has sent more children to Carmichael’s service than the whole of Greater London — although it has half the population.
Professionals are under pressure. A Brighton teacher said: “What’s happening is worrying and many of us know it, but nobody wants to speak up and get shot.” The NHS gender service is caught between the demands of groups such as Mermaids, which want children given cross-sex hormones before they turn 16, and women’s campaigners, who accuse it of already bending too far to activists.
Many clinicians are simply affirming of these increasing numbers of trans identified females. Rather than ask questions, their attitudes are celebratory. The below quote from the same article reflects this common attitude among educators, “LGBT” organizations, therapists, and media:
He said: “In the last years I have visited many schools in Brighton and they have support programs for LGBT students and curriculum about gender diversity. It’s great to see schools are active in supporting students in their journey.”
Body hatred, psychosomatic illnesses, mass psychogenic illness, mass hysteria, and mass delusions can be socially contagious, and more so in females, particularly pubertal ones. They are more prone to this than any other demographic (see below). And in response to the rapid increase of gender dysphoric females coming to gender clinics, some are exploring the social contagion factor involved in what is being called “rapid onset gender dysphoria” or ROGD. In the past, many of the females in gender clinics were very gender nonconforming and expressing distress around their gender from a young age. The youths who remained highly dysphoric into the teenage years were then considered for medical transition based on a solid screening process.
Many in the new wave of gender dysphoric adolescent females did not have distress, or even any gender non-conforming behavior, in childhood. The realization comes more suddenly and is reinforced by an online, pro-trans, and a pro-medical body modification culture. This pro-transition attitude is promoted by therapists, schools, the media, and “LGBT” organizations. What is going on here?
1) The affirmative model lobby argues that more young females are coming out due to more social awareness and acceptance. The tween females are experiencing the intense dysphoria suddenly due to the onset of secondary sex characteristics in puberty. They seek out other females who feel the same as they do on the internet, and in peer groups, which would be expected. Adult females can also come to the realization they are dysphoric after, in most cases, identifying as lesbians for years. So, a later realization of transness should not be considered invalid.
2) Those who are affirmative model skeptics argue that transitioning so many young girls, at a time when most girls experience discomfort and distress about their changing body, and before full maturity and identity development is irresponsible. Also, experiencing distress around puberty is very common among lesbians, who have resolved this in the past without medical intervention. Many females don’t go seeking information about GD online. They get exposed to it and latch on to it as an explanation as to why they feel different from other girls possibly due to autism or lesbianism. They then latch onto medical transition as a panacea to cope with their normal bodily discomfort during puberty and finding social belonging. Skeptics believe the internet fuels this. The online environment glorifies body dysmorphia (there are 1000’s of transition and GD videos/blog posts) and a youth rebellion culture that goes along with it. Social acceptance and trans visibility do not fully explain the huge sex ratio discrepancy in youth compared to adults. There should be an equal number of males coming out younger.
The pro medical argument is certain to be true for some cases. And some people do realize they want to transition later in life. It is very possible the second scenario is also unfolding for some of these young people. This puts them at risk of over-medicalizing their gender dysphoria when they are still immature, with permanent consequences. Even though there are people who come to an understanding of themselves as teens or even adults, some young people’s own descriptions of their experience support social contagion being a factor in their trans identification. Therapists treating young people should be aware of this, although many are not, as parents are finding much difficulty finding mental health professionals who don’t recommend immediate transition.
Lisa Marchiano, a Jungian analyst, Ph.D. and therapist who has communicated with many parents, trans adults, and detransitioners in her publication, “Outbreak: On Transgender Teens and Psychic Epidemics” has this to say:
This transgender trend looks strikingly like other social contagions to which adolescents are known to be prone. There is considerable research on suicide contagion among teenagers. There is also a great deal of research on social contagion in eating disorders. To take just one example, Paxton et al. demonstrated that a teen girl’s use of extreme weight-loss behaviors is closely linked with whether her friends use them.
Susan Bradley, a psychiatrist and expert in autism and gender dysphoria, agrees that these rapid onset cases need to be examined more closely, beyond simple enthusiastic affirmation.
In my own practice, I have seen a good many young women displaying the phenomenon known as “rapid onset gender dysphoria,” or ROGD, which overwhelmingly affects girls.
Typically, the ROGD teenage girls I see have, wittingly or not, begun to experience homoerotic feelings about which they are conflicted. They tend to be socially isolated, and somewhere “on the spectrum.” They may have histories of eating or self-harm disorders.
They have found companions with the same attributes on Internet sites, which diminishes such adolescents’ sadness over their social isolation, but which can also lead to foreclosure of reflective thinking about their own feelings and situation. Some of these girls are depressed, afflicted with suicidal idealization. Because of the initial euphoria they experience in finally “belonging” to a well-defined kinship group, they tend to embrace the idea of transitioning wholeheartedly as the solution to their other problems.
Parents of ROGD girls find themselves in uncharted or even hostile territory if they resist the affirmative model, which is now the default position in schools, social service programs and gender-focused clinics. As they are often told their daughters may commit suicide if they are not affirmed and encouraged, these parents struggle to find an approach that is safe for their daughters without compromising their own well-founded skepticism and protective instincts. They are rightly alarmed by the speed with which gender professionals glide from (near-instant or even self diagnosis to recommendations for off-label and lightly studied hormone blockers or cross-sex hormones (which cause infertility).
What evidence is there that the rising levels of GD in females may be related to wider issues of female dissatisfaction beyond a conflicted “innate” gender identity? There are many other historical examples of social contagions of self-harm, delusions, psychosomatic illnesses, and conversion disorder, mainly affecting females, that support the above concerns are valid. Here are just some of the many examples of historical social contagions, some of them very bizarre. Many happened earlier in history without mass social media.
1) The spread of bulimia:
As bulimia gained further diagnostic legitimacy in 1980 with its inclusion in the third edition of the Diagnostic and Statistical Manual of Mental Disorders, Russell ruefully tracked its unexpectedly swift spread across Europe and North America, where it infiltrated college campuses, affecting 15 percent of female students in sororities, all-women dormitories, and female collegiate sports teams. The disease moved through the halls of American high schools, where binging, fasting, diet pill use, and other eating disorder symptoms easily clustered. He chased its dispersion across Egypt, where the number of new cases grew to 400,000. In Canada, it swelled to 600,000. In Russia, 800,000. In India, 6 million. In China, 7 million. In the UK, one out of every one hundred women was now developing the disorder.
With this knowledge, Russell’s discovery took on characteristics of a pandemic that was set to claim 30 million people, but neither he nor anyone could do a thing at that point to stop it. He was confronted, he says, by a problem of entropy, a gradual decline into disorder with devastating implications for social contagions: once they are out, they are virtually impossible to rein back in.
Another example of socially contagious body dissatisfaction happened in Fiji:
Just a few years after the introduction of television to a province of Fiji's main island, Viti Levu, eating disorders -- once virtually unheard of there -- are on the rise among girls, according to a study presented yesterday at the American Psychiatric Association meetings in Washington. Young girls dream of looking not like their mothers and aunts, but like the slender stars of ''Melrose Place'' and ''Beverly Hills 90210.”
Fifteen percent in the 1998 survey reported that they had induced vomiting to control their weight, the researchers said, compared with 3 percent in the 1995 survey. And 29 percent scored highly on a test of eating-disorder risk, compared with 13 percent three years before.
A similar situation unfolded in Japan:
2) Socially contagious anorexia:

3) A very recent and large spike in labiaplasties:
Another phenomenon currently happening alongside the large upswing in females going to gender clinics, and binding their breasts, are teenage girls and women having their labia surgically cut to adhere to porn star esthetics. Pornography is something young males and females are exposed to on a wide scale in this point in history. Labia dysphoria was unheard of in the past. The problem is serious enough that in Britain, the Royal College of Obstetricians and Gynecologists have had to implement a public health response, and girls as young as nine years old are being affected according to this article:
In 2015-16, more than 200 girls under 18 had labiaplasty on the NHS. More than 150 of the girls were under 15.
Some experts fear that pornography and images viewed through social media are leading young girls to have unrealistic perceptions of how their genitals should look.
Girls will sometimes come out with comments like, 'I just hate it, I just want it removed,' and for a girl to feel that way about any part of her body - especially a part that's intimate - is very upsetting.
4) The Needle girls:
The “needle girls” was a term applied to young females caught up in a self-harming epidemic in the late 1800’s:
An NPR program, “The History and Mentality of Self-Mutilation” noted that in the late 19th century, two American doctors described a strange phenomenon. Women were puncturing themselves with sewing needles. The practice was so common, that doctors began to refer to the so-called “hysterical” women who did this as “needle girls.”
Self-embedding is still happening today:
Some doctors are alarmed by what they see as a growing trend by adolescents to mutilate their bodies through "self-embedding" -- inserting shards of wood, glass or paper clips under their skin.
Other medical experts, however, claim the embedding of needles and other objects in the skin is not a new syndrome, but is part of a growing problem of self-injury that is gaining attention...
Dr. Armando Favazza, author of the book "Bodies Under Siege" and a professor of psychiatry at the University of Missouri-Columbia, has found evidence of a spontaneous self-embedding trend in early 19th century Europe.
"Back in 1896 psychiatrists compiled medical reports on women [they labeled them all as hysterical] who stuck pins in their bodies," said Favazza.
Just like Shiels presented Dec. 3, doctors in the 1890s presented X rays of women with needles, sometimes hundreds, embedded in their skin.
"It was a cultural influence that produced these 'needle girls," said Favazza. "There was a lot of fascination with holy men in the Near East … and entertainers."
5) A mass hysteria spread where girls were afraid they were being sprayed with poison gas through their windows:
6) A mass psychogenic illness in Mexico:
In 2006, a mysterious illness began to affect girls at a boarding school in Chalco, Mexico, near Mexico City. The school, which is run by Roman Catholic nuns, is one of 10 in Asia and Latin America operated by a charity called World Villages for Children in Asia. The girls, ages 12 to 17, showed strange symptoms: difficulty walking, fever and nausea. After the girls returned from a 10-day Christmas break, the illness spread. Eventually 600 out of the 3,600 girls at the school showed symptoms.
7) A mass psychogenic illness in Ripon:
Like the Lancashire mill incident, the events at Outwood academy bear the hallmarks of what was once called mass hysteria, but which is now called mass psychogenic illness (MPI). Doctors have recorded cases for hundreds of years and fresh incidents crop up around the world most weeks. “This is incredibly common and happens to completely normal people,” says Simon Wessely at the institute of psychiatry, at King’s College London, who wrote his first paper on the subject in 1987.
8) A mass psychogenic illness in Danvers:
About two dozen teenagers at the Essex Agricultural and Technical School began having “mysterious” hiccups and vocal tics.
Though the Massachusetts State Health Department still has not declared the Danvers outbreak to be MPI, back in March, Bartholomew said, “[Danvers] could turn into another Le Roy, if they don’t watch their step.” Typically, mass hysteria is confined to a group of girls or young women who share a common physical space for a majority of the time. Bartholomew has studied over 600 cases, dating back to 1566, and said that the gender link is undeniable; it’s just a question of why. It is accepted within the psychiatric community that conversion disorders are much more common in females. There are also social, biological, and anthropological theories that have to do with how and why females might cope with stress.
He was referring to an episode of mass hysteria in Le Roy, a small town in western New York, that garnered massive media attention in the winter of 2011 when about 18 girls at the local high school came down with a very dramatic—and very real—case of hysteria. Bartholomew said that the Danvers case looks extremely similar to the case in Le Roy and that the lessons from Le Roy have gone “unheeded.”
The June bug epidemic serves as a classic example of hysterical contagion. In 1962 a mysterious disease broke out in a dressmaking department of a US textile factory. The symptoms included numbness, nausea, dizziness, and vomiting. Word of a bug in the factory that would bite its victims and cause them to develop the above symptoms quickly spread.[2]
Soon sixty-two employees developed this mysterious illness, some of whom were hospitalized. The news media reported on the case. After research by company physicians and experts from the US Public Health Service Communicable Disease Center, it was concluded that the case was one of mass hysteria.
10) A mass psychogenic illness in in Leroy
11) A group of Fainting school Girls”
12) Witch trials, who many people are aware of:
Charles Mackay, in Memoirs of Extraordinary Popular Delusions: The Madness of Crowds, recounts a particular incident (in the middle of a continent wide mass delusion that killed massive amounts of innocent people) that involved 50 girls believing they were witches.
A singular instance of the epidemic fear of witchcraft occurred at Lille, in 1639. A pious but not very sane lady, named Antoinette Bourignon, founded a school, or hospice, in that city. One day, on entering the schoolroom, she imagined that she saw a great number of little black angels flying about the heads of the children. In great alarm she told her pupils of what she had seen, warning them to beware of the devil whose imps were hovering about them. The foolish woman continued daily to repeat the same story, and Satan and his power became the only subject of conversation, not only between the girls themselves, but between them and their instructors. One of them at this time ran away from the school. On being brought back and interrogated, she said she had not run away, but had been carried away by the devil; she was a witch, and had been one since the age of seven. Some other little girls in the school went into fits at this announcement, and, on their recovery, confessed that they also were witches. At last the whole of them, to the number of fifty, worked upon each other’s imagination to such a degree that they also confessed that they were witches–that they attended the Domdaniel, or meeting of the fiends–that they could ride through the air on broomsticks, feast on infants’ flesh, or creep through a key-hole.
From the Guardian:
In the Middle Ages, Wessely notes, local priests were called in to exorcise demons, a tough task with so many believing in witchcraft. “They were fortunate in one regard: they did not have to contend with mobile phones, Twitter or Facebook.”
Dancing plague involved people dancing nonstop for days on end. Some dropped dead of exhaustion.
The outbreak began in July 1518 when a woman, Mrs. Troffea, began to dance fervently in a street in Strasbourg.[1] This lasted somewhere between four and six days. Within a week, 34 others had joined, and within a month, there were around 400 dancers, predominantly female. Some of these people would die from heart attacks, strokes, or exhaustion.[1] One report indicates that for a period, the plague killed around fifteen people per day.
14) The recovered memories (of child sexual abuse) scandal:
There was an epidemic of false sexual abuse accusations that happened in the 1980’s and 1990’s. These included individuals and organizations being accused of satanic rituals such as daycare centers and accusations of sexual abuse family members. Memories of such abuses were often recalled in therapy. These accusations were so common two organizations had to be formed by families in Britain alone to challenge them.
“Families are still living the nightmare of false memories of sexual abuse”:
The occasion in question was the 15th Annual General Meeting of the British False Memory Society (BFMS). The BFMS began life in 1993, the year after the formation of the False Memory Syndrome Foundation in the US. Accused parents were at the forefront of founding both organizations. Both have scientific and professional advisory boards to support them in their aims, which include providing support and legal assistance where necessary – to those affected by such accusations, providing information and advice to professionals, and improving our understanding of false memories by encouraging and support academic and professional research.
Most accusers were females:
The nightmare was just beginning. Repressed memories were surfacing everywhere. In June 1991, Marilyn Van Derbur, a former Miss America, told the world that at age 24, she had discovered her father's sexual abuse of her as a child. Later that year, Roseanne Barr claimed to have recovered 30-year-old memories of both parents molesting her. ("He used to chase me with his excrement and try to put it on my head," she said of her father.) Women were suing their parents for millions of dollars. Hundreds of accused families sought help.
15) Socially contagious cutting among females:
Cutting behaviors have been reported for many years and are on the rise, reaching epidemic proportions (Froeshcle & Moyer, 2004), but there is no hard and fast evidence as to why. Concern is at such a fevered pitch that the American Self-Harm Information Clearinghouse named March 1, 2005 as National Self Injury Awareness Day to educate and inform medical and mental health professionals and the general public about self injury. The United Kingdom and Australia have marked March 1st as National Self-Injury Awareness day in their respective countries as well.
Media contagion seems to be a common theory as to why cutting is on the rise. High profile individuals like Princess Diana, Johnny Depp, Christina Ricci, Fiona Apple, Angelina Jolie and Courtney Love have revealed that they deliberately cut or self injured. Movies like “Girl, Interrupted” and “Thirteen”, depict individuals using cutting behaviors as a means to reduce adversity. This gets translated as a possible option for individuals who are grappling with significant emotional turmoil. Peer contagion is also a factor in school and work settings - If she tried it, maybe this can work for me.
Another example:
It started as an impulse. Of course I know a lot of girls who cut so the idea came to me and I started with a paper clip. I ran it along the inside of my arm until it made a mark. Then I went deeper until I made myself bleed. It was totally engrossing and I can’t explain why but it made me feel better. I graduated to straight edge razors and, at the time, it seemed perfectly fine to me. It was a little secret compartment of my life where I had all the power and control.
While self-harming is not a new phenomenon, this particular offshoot is showing a disturbing rise in popularity. Accurate statistics are hard get but if you ask a professional who works with teen girls (therapists, counselors, teachers, coaches); you are likely to hear it is becoming more and more common.
There have been many other cases of physic epidemics, psychosomatic illness, and mass hysterias in the past with a majority of such cases involving young females. In regards to mass psychogenic illnesses in particular PhD Robert Bartholomew has noted:
‘of the 2,000+ cases in my files which date back to 1566, this pattern holds true over ninety-nine percent of the time.’
And:
Francois Sirois analyzed 45 school outbreaks from around the world, and found that girls near puberty are most frequently affected. Sirois observes that outbreaks in Western schools, affect girls at about the same rate as those in other parts of the world, despite the social conditions being fairly uniform for both sexes. Many psychogenic conditions are more common in females, including individual cases of conversion disorder, and globus hystericus, a feeling of a lump in the throat that produces a sensation of choking.
There have been multiple articles in the last few years discussing how social media in particular can fuel these social contagions. This article discusses that self-harming and poor mental health in teenage girls are in fact influenced by social media.
Prinstein, whose research focuses on the role of social influence on adolescent self-injury, suggests websites that discuss how to do it, similar to those that promote eating disorders, may be contributing to the spread of the behavior. Certain celebrities have also been widely reported to have engaged in self-harm, including actress Angelina Jolie and comedian Russell Brand. And teens are also learning about self-harm from one another.
Knowing that others engage in the behavior may increase the incidence, since teens are at a developmental stage that makes them particularly susceptible to peer influence,Prinstein says. But it's not just the act of self-harming that appears to be contagious. He says the feelings of anxiety and depression that prompt young people to hurt themselves may be socially transmitted as well.
Amanda Rose, a professor of psychological sciences at the University of Missouri, suggests "co-rumination," or the sharing of problems and negative thoughts, is to blame. She and other researchers have found growing evidence that co-rumination, especially among teenage girls, can undermine mental health.
Citations can be found here to verify the negative impact on mental health of co-rumination with depressed/anxious peers. This phenomenon is amplified by access to thousands of others on social media. The study below focuses on rumination in girls:

Social media and its power to drive social contagions are also discussed in this Atlantic article. “What Witchcraft is Facebook.”
One major lesson missed: the power of social media to spread and exacerbate an episode…
According to Bartholomew, there is “potential for a far greater or global episode, unless we quickly understand how social media is, for the first time, acting as the primary vector or agent of spread for conversion disorder.” He believes that epidemics spread by social media are “inevitable” and that “it's just a matter of time before we see outbreaks that are not just confined to a single school or factory or even region, but covering a disperse geographical area and causing real social and economic harm.”
Catching an illness through Facebook sounds wonky. But the contagion of hysteria relies, among many things, upon the unconscious interpretation of what is suggested to us. Fitzsimmons did not even have to be in physical contact with the other girls to “catch” their disease. Marge encapsulates the power of social media to penetrate and trigger actions of the unconscious mind. She marks “a historical shift in terms of the trigger for people being affected and sucked into these cases,” Bartholomew said.
Parents are reporting they cannot get mental health counseling for their minor children because therapists are viewing all of their child’s problems as being related to not being able to transition. Body hatred issues and self harm such as cutting in those experiencing GD may not be solved by an affirmative model approach by parents and health professionals. This youth committed suicide even with much outside support for transitioning. It would be in everyone’s interest to find out exactly the best way to help these young people to stop this. Perhaps there needs to be more of a focus on coping with negative rumination and learning emotional regulation rather than medical treatment.
if I die…I don’t want to be remembered as the faggot gay girl with all the scars on her arm. unfortunately that’s who I am to a lot of people. if those people would have just stayed silent and kept their ignorant thoughts in their heads then maybe i wouldn’t have those scars on my arm. maybe. it wasn’t always about what they had in their heads, it was what was inside of mine to. i just didn’t understand why i felt the way i did when i had a decent life. i may have come from a broken family but i always had a roof over my head and a loving mother who fully accepted me for who i was and never stopped trying. she was the only person who never gave up hope on me. but anyway, i don’t want to be remembered as the girl with problems, just remember me as someone who understood and stayed strong for as long as i could.
There are anecdotal examples and general observations by individuals who believe social contagion is influencing young people, females in particular, to identify as transgender. Every trans student in this Australian school happens to be female and this appears to have evolved after transgender trainings in schools,
Official statistics are tightly held but, anecdotally: one public school in Sydney’s eastern suburbs has five transgender children, according to the relative of a student; a regional NSW government Safe School had five transgender students at the start of last year, according to a former teacher; a Safe School in outer Sydney had 5 or 6 “transgender” children last year in Year 8, all girls, according to a concerned teacher. “Safe Schools definitely had something to do with all this,” he says. “We are losing this fight… very badly”.
Below is a list quotes from parents commenting about trans identification as a social phenomenon:
-Recently I was talking to a therapist friend who specializes in LBGTQ teens. I told her what was going on, but said I was skeptical. I was expecting her to talk me down, and tell me why it’s important that my husband and I embrace J’s declarations and enable her. Instead she told me the therapy community is having to dial back on what seems to be an “outbreak” of transgenderism, and to approach the subject with more skepticism. That was enough for me, for now.
-This has happened with my daughter as well. She fell into an online group and suddenly became convinced she was transgender. She wanted us to call her a male name and pronouns, asked for a binder, testosterone and planned for a double mastectomy. She was persistent for about a year. But she eventually decided she wasn’t transgender after all. She admitted that she was confused. Now she is back to feeling female again.
-I totally agree with the author that it is very trendy for kids now to suddenly come out as transgender. This isn’t transphobic to admit. It is really happening. At my daughter’s high school there is a whole group of girls that feel they are some variant of gender, pretty much anything but female.
More parents commenting on this Washington Post article, demonstrating schools and therapists are very enthusiastic about immediately affirming and transitioning young people:
-It’s easy to think this is fine - until they come for your daughter. I’ve been through my daughter being sucked into this cult. She only felt “trans” for three months. In that time her school was already proposing changing her name and pronouns. Too fast! It’s a fad. She now says she isn’t interested any more. She’s 14 and felt awkward about her body - as I did at that age.
-I had previously been virtue signaling on the transgender civil rights movement - thinking I was just being loving and tolerant. Then at age 12, my daughter said she was a boy - boom! - there was no warning, no signs, no history of any gender dysphoria - and she didn't "hide it" because she as a child, her speech was like a stream of consciousness! I knew in my gut that this wasn't right. But she was so convincing. She started saying she always felt this way. She convinced her therapist who followed the treatment guidelines of affirmation therapy. We supported her sexual orientation questioning without so much as a blink, but this was something we had to think about. Fast forward to a year and a half later (which was pure torture), she says she is a happy girl. She says that "I began questioning why I felt so awkward in my body and why I hated myself.” She says, “…I started watching people on YouTube that felt the same way I did. I would watch them in envy as they talked about their binders and whatnot.” She says, “I hated my chest. I can’t explain why, but I hated them so much. I wore baggy clothes to hide them….. I wanted them off so bad…” A turning point came for her and she says, “I realized that I just wanted a reason for the way I felt, that the second I found this seemingly possible solution, I grasped onto it and wouldn’t let go. It seemed like the perfect solution; it came with something to fight for as well. There were others like me, and it felt good to finally belong somewhere….But now I was realizing that this was not the solution. I was suddenly grateful that I had not transitioned. It would have ruined me.” If people can’t understand how this is happening right this very moment and not being reported due to worries about being called a bigot or transphobe, then you haven't bothered to stop and think how vulnerable preteens and teens are to this rapid medicalization approach. Something needs to change ... and it wasn't my daughter.
More parental observations:
My daughter’s gender therapist fully and nonchalantly agreed with my observation that groups of girls are doing this: entire friend groups!…



Some young people themselves recognize social influence as a factor.
My 19-year-old daughter said to me “I know there are girls just doing this and they are not really trans but I REALLY AM!!”
A previously trans identified female on he autism spectrum believes social contagion is a factor (8:40-8:53).
I know that some of you have identified your daughter’s dysphoria as social contagion and I agree that the exponential increase in females presenting at gender clinics represents an element of that.
Because of this well-established historical evidence on social contagion and females, some doctors and therapists are worried,
Both doctors agree with James Caspian, a Jungian, who calls this trend in girls “a collective complex”, a form of mass hysteria fed by online communities. Tumblr and Reddit brim with transition webpages, support groups of girls egging each other on, celebrating when they start “T” (testosterone). As an experiment, I took several “Am I trans?” questionnaires, giving the most ambivalent answers. The result is always “probably” or “yes”.
Tania Marshall, an autism expert who has encountered females with GD including desisters and regretters, worries about glamorization of gender dysphoria and medical transition presented online to impressionable young people.
Some of them have said to me that they watch famous YouTubers who’ve transitioned and their life just looks so fabulous. You know, like people’s life on Instagram. They’re following these people who seem to have wonderful lives on YouTube, or Instagram, or Twitter. And it reinforces them to proceed with taking hormones and transitioning. So, they see these YouTubers who’ve transitioned as their role models. But they fail to see that the YouTubers, or Instagramers, or whoever are putting their best face on. They often believe their anxiety and depression will go away if they transition. So, not feeling like a girl in the teen years, being highly influenced by social media, can bring on that sudden belief that they’ve been born into the wrong body. And they need to change to a male to be happy. They romanticize about it. They believe that becoming a male will solve all of their problems.
Lisa Littman explores the possibility of social contagion:
There are many insights from our understanding of peer contagion in eating disorders and anorexia that may apply to the potential peer contagion of rapid-onset gender dysphoria. Just as friendship cliques can set the level of preoccupation with one’s body, body image, weight, and techniques for weight loss [28–30], so too may friendship cliques set a level of preoccupation with one’s body, body image, gender, and the techniques to transition. The descriptions of pro-anorexia subculture group dynamics where the thinnest anorexics are admired while the anorexics who try to recover from anorexia are ridiculed and maligned as outsiders [30–32] resemble the group dynamics in friend groups that validate those who identify as transgender and mock those who do not. And the pro-eating-disorder websites and online communities providing inspiration for weight loss and sharing tricks to help individuals deceive parents and doctors [33–35] may be analogous to the inspirational YouTube transition videos and the shared online advice about manipulating parents and doctors to obtain hormones…
The following case summaries were selected to illustrate peer, trauma, and psychiatric contexts that might indicate more complicated clinical pictures.
-A 12-year-old natal female was bullied specifically for going through early puberty and the responding parent wrote “as a result she said she felt fat and hated her breasts.” She learned online that hating your breasts is a sign of being transgender. She edited her diary (by crossing out existing text and writing in new text) to make it appear that she has always felt that she is transgender.
-A 14-year-old natal female and three of her natal female friends were taking group lessons together with a very popular coach. The coach came out as transgender, and, within one year, all four students announced they were also transgender.
-A natal female was traumatized by a rape when she was 16 years of age. Before the rape, she was described as a happy girl; after the rape, she became…
-A 14-year-old natal female and three of her natal female friends are part of a larger friend group that spends much of their time talking about gender and sexuality. The three natal female friends all announced they were trans boys and chose similar masculine names. After spending time with these three friends, the 14-year-old natal female announced that she was also a trans boy.
-withdrawn and fearful. Several months after the rape, she announced that she was transgender and told her parents that she needed to transition.
An affirmative model skeptic highlights the relevant quotes (Kaltiala-Heino 2018) pertaining to this issue in Scandinavia and elsewhere.



These questions need to be addressed by responsible mental health and medical practitioners to insure therapists and doctors do not inappropriately misdiagnose and transition minors, which could harm young people and result malpractice lawsuits. The legal ramifications should perhaps concern these professionals in light of mounting accounts of female teenagers desisting from gender dysphoria. The youths below met the criteria for a DSM-V diagnosis of gender dysphoria, despite outgrowing it. They would have met standards for medical transition and even surgery in the United States.
Comments from parents on a gay supportive but affirmative model skeptic website (4thwavenow):


A Facebook comment:

More quotes pointing to peer influence in gender dysphoria may be found in this blog post from a mother whose teen daughter desisted from gender dysphoria. Her informal social media survey shows a majority of parents who responded had female children.

lilymaynard (Wordpress censored this blog and removed it)
Often mass psychogenic illnesses will quickly resolve but social contagions involving eating disorders and self-harming do not resolve quickly and become endemic in the culture. If social contagion is a factor in trans identification in female youth, it will most likely continue to influence young females in the future, as this additional body dysmorphia becomes imbedded in the culture.
An interesting blog post presents arguments as to why the comparison of trans people coming out to homosexuals coming out is not appropriate
It’s this ratio that most clearly illustrates the social contagion aspects of the modern transgender condition. Not only has the prevalence of transgender symptoms soared, the ratio has completely reversed, with 3 young female patients seeking reassignment to a more masculine presentation for every 1 male patient seeking feminization.
Not one sex researcher in history — not one, and if you find one, comment here and I will append this immediately — found that more females wanted to change sex than males. Not in any country, not in any age group. Not until the social contagion phenomenon known as ROGD, or rapid-onset gender dysphoria, began.
Another factor to note is that numbers of trans identified females are going up and that there are many more bisexual and heterosexual females medically transitioning. This is becoming more common because of cultural exposure. Many of these individuals likely never would have considered medically transitioning in the past, as these surgeries and hormones have been available for years to any persons with an “innate” gender identity.
Psychologists Ray Blanchard and Michael Baily discuss heterosexual female FtMs here, whose numbers are increasing:
For the sake of completeness, we include two other kinds of gender dysphoria. We suspect that both are rare, even among persons with gender dysphoria. One of us (Blanchard) has seen cases of the first type, autohomoerotic gender dysphoria, which appears to be an erotically motivated gender dysphoria. In this case, sexually mature natal females (i.e., not biologically still children) become sexually preoccupied with the idea of becoming a gay man and interacting with other gay men.
…For example, a female with rapid onset gender dysphoria may be sexually attracted to males and thus strive to become a gay man, similar to autohomoerotic gender dysphoria. The important difference is that the female with rapid onset gender dysphoria is not primarily motivated by an erotic desire to be a gay man. Instead, having the prospect of having sex with gay men is a by-product of her condition, not the main point of it.
Others do believe in an autohomoerotic component to heterosexual females who want to be gay men. There are more examples of heterosexual females who are transitioning and identifying as gay in the media. There is in fact, a proliferation of this subculture on social media sites like Tumblr (see why so many females). Some describe it as the reverse of autogynephilia, and note a connection with anime and sexually provocative material. More research is needed on how social media may affect sexual orientation (there are many more bisexuals now) and gender identity.
More information on social factors and trans identification see here.
C. Mental Illness
Almost all studies on trans youth and adults show high rates of comorbid mental health conditions. A more complete review of mental health information may be found here and here.
This large scale study done on trans youth by a health insurance company shows these youths tend to have many other mental health problems.
“We looked at mental health in transgender and gender-nonconforming youth retrospectively between 2006 and 2014 and found that these youths had three to 13 times the mental health conditions of their cisgender counterparts," said the study's lead author, Tracy A. Becerra-Culqui, PhD, MPH, of the Kaiser Permanente Southern California Department of Research & Evaluation. "Among these young people, the most prevalent diagnoses were attention deficit disorders in children, 3 to 9 years of age, and depressive disorders in adolescents, 10 to 17 years of age."
Anxiety and depression would be expected to be higher in marginalized populations. However, studies on trans youth often show there are several other issues such as ADD, BPD, OCD or autism. These are problems that would not necessarily be related to the stress of being gender nonconforming.
Attention deficit disorder (transfeminine: 15 percent, transmasculine: 16 percent). These numbers are 3 to 7 times higher than the matched cisgender reference group.
Given the reality body dysmorphia issues are common in females (covered extensively in the previous section), some mental health professionals are worried that females with BDD are being misdiagnosedand and affirmed as transgender.
We are following a series of protocols with gender-dysphoric children, who may in fact be body dysmorphic. We may be doing exactly the wrong thing, if that diagnosis is wrong. We are working in the dark, experimenting on children.
Observations for the GIDS in Britain seem to validate his concern, especially in natal females.
For the children who commenced the blocker, feeling happier and more confident with their gender identity was a dominant theme that emerged during the semi-structured interviews at 6 months. However, the quantitative outcomes for these children at 1 years time suggest that they also continue to report an increase in internalising problems and body dissatisfaction, especially natal girls.
A gender clinician believes the mental health issues are central to the increase of trans identification and may not just be a result of the gender dysphoria itself. This viewpoint is now sometimes censored and shamed in the mental health profession.
Megan, who works at a clinic in Sydney with young people, aged from 12 to early 20s, who have asked for referrals for sex changes, says: “Often, especially with females, there’s child abuse in their background, a lot of mental health issues and challenges. The system I work in does push that process. You’re not able to say this is a psychological issue. There’s this push to refer them out and get them processed to [send them to] Westmead children’s hospital and into that [sex change] process.
Another father from the same article talks about mental illness being the primary factor in his daughter’s trans identification.
One father, Gus, tells of “the most terrifying day of my life”, when he picked up his 16-year-old daughter from school, and “she didn’t know where she was, she wasn’t the full quid, she was just really confused... We went to the doctor [and] just out of the blue she said she was a boy in a girl’s body.”
It turned out “she was going through a psychotic episode. She was in hospital for two months… She’s just a normal girl now ... It was all purely a mental health issue.”
Canadian researchers note high rates of comorbid conditions in youth in a trans accepting country at a trans affirming clinic indicating issues beyond failure to affirm “innate gender.” Again, high rates of girls and same-sex attraction are noted.
The paper examines the case files of 17 people assigned a male gender and 33 people assigned a female gender, at birth, based on their biological sex. Following their experience of gender dysphoria, the clients had been referred to a specialist gender identity service for young people, at which time they were aged 13 to 20. Sixty-four per cent of the clients were homosexual with respect to the gender they were assigned at birth.
This article provides two examples of females from the study with mental health problems not served by transition, but were aided in transition by enthusiastic professionals.
In both these cases, after an initial assessment the individual was given testosterone treatment by a physician against the wishes of the parents – in the first case, the physician actually refused to meet the parents, and in the second, the physician recorded that the issues raised by the parents regarding anxiety, sexual and social problems weren’t relevant for the course of action. Sadly, in the case of the second individual, a few months after the start of the hormone treatment, they made a suicide attempt that required hospitalisation; the reasons for this were not reported.
Finland is a country with a small population but currently has the largest female to male ratio of 7/1. Since transgender issues are on the internet, and discussed in public, it is worth looking at what is going on with this population and determine if other mental illnesses are fueling the trans identification in a way that would not have happened twenty years ago.
In the majority of the applicants, gender dysphoria presented in the context of wider identity confusion, severe psychopathology and considerable challenges in the adolescent development. At this point it is not possible to predict how gender dysphoria in this group will develop:
The recorded comorbid disorders were thus severe and could seldom be considered secondary to gender dysphoria. This utterly contradicts the findings in the Dutch child and adolescent gender identity service, where two thirds of adolescent SR applicants did not have psychiatric comorbidity.
Gender dysphoria seems to be rising along with other mental health problems in females. The biggest uptick in mental deterioration is among teen girls in this US study that shows similar results to the recent British study mentioned above. Much of this rise is being blamed on social media.
A steady increase in admissions due to suicidality and serious self-harm occurred at 32 children's hospitals across the nation from 2008 through 2015, the researchers found. The children studied were between the ages of 5 and 17, and although all age groups showed increases, the largest uptick was seen among teen girls.
In 2008, about 60% of all children and teens hospitalized as a result of suicidal thoughts or attempts were girls, and, by 2015, that number had increased to 66%, said Plemmons. While he did not break down age groups, he said the Centers for Disease Control and Prevention reported that suicides had tripled in girls, ages 10 through 14, between 1999 and 2014.
Lisa Marchiano talks about mental illness being an identity reinforcing behavior and that trans identification may be following this pattern in some individuals.
Social contagion among teens is a rich area of literature for which many examples could be cited. This 2014 study found that teens who adopt an “alternative” identity such as “emo” or “Goth” were more likely to self-harm. This was true even after controlling for other factors. The authors point out that engaging in self-harm aids in reinforcing group identity among teens.
D. Abuse
Physical and sexual abuse appear to influences gender dysphoria in newer cases of females presenting with gender dysphoria. Transition may appear to be a solution to feelings of victimization, and girl/women victimization in particular. A recent study on gender dysphoric young females shows high rates of past trauma.
From the Economist on “Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports”:
Dr Littman thinks that some adolescents may embrace the idea that they are transgender as a way of coping with symptoms of a different, underlying issue. Almost two-thirds of the children had one or more diagnoses of a psychiatric or developmental disorder preceding the onset of gender dysphoria; nearly half had self-harmed or experienced some trauma.
According to this Australian clinician:
Often, especially with females, there’s child abuse in their background.
Another Australian clinician notices the same pattern,
Psychiatrist Dr Stephen Stathis, who runs a gender clinic, said he had seen girls who had been sexually abused and wanted to identify as transgender.
Here a detransitioner herself says that sexual abuse contributed to her gender dysphoria:
I’m a biracial 20-something from the US…To summarize my situation: I was severely dysphoric and transitioning to male seemed right for me– in fact it seemed like the only option for me other than death. However, when I moved out of my sexually abusive father’s house– having lived as an FTM for several years with zero doubts, having gotten a double mastectomy, changed my legal name and gender, and having taken hormones for 2 years– my desire to be male instantly vanished and was replaced by equally intense dysphoria because my body no longer looked female. In hindsight, I probably should have addressed my sexual trauma before permanently changing my body!
After I detransitioned, several other FTMs I knew from the queer youth group I had been a part of also detransitioned. Two of them told me that seeing me publicly detransition made them realize that it was okay for them to do the same. I was very close to one of the detransitioners in our cohort and she told me that her transition had also been related to a history of sexual abuse that she’d never spoken to her therapist about. I think another told me something similar, but for some reason I can’t remember who it was. I discovered online that there were many other women who had transitioned to male because of unaddressed sexual trauma that later re-identified as female.
Another account of a detransitioned FtM indicates trauma from abuse was a factor in her desire to transition,
…Angela*, was also an abused child. Sexually molested by a cousin between the ages of four and nine, she grew up hating her femininity.
She recalls punching her breasts and working out obsessively at the gym to "remove anything that reminded me I was female". She was a 22-year-old university student when she was referred to the clinic by her GP, depressed and struggling with her identity. Dr Kennedy diagnosed her as transsexual at the first assessment, prescribing her male hormones and suggesting female-to-male surgery.
Within months Angela's body was covered in thick hair, her voice deepened and she had a full beard. She had to shave under the covers every morning to hide the truth from her conservative Catholic parents. Two years later she had surgery to remove both breasts and was scheduled to have a full sex change. Angela could no longer conceal the truth from her family and began living as "David". Thankfully, she says, she realised there had been a mistake before undergoing full genital surgery.
"I remember at one point looking at myself in the mirror with this beard, my breasts gone and thinking, 'Oh my God, what the hell am I going to do?' … I felt ugly. I was the classic bearded woman, a monster trapped between two worlds."
She claims her pleas for help were also ignored by the clinic and her return to life as a woman was a nightmare that involved two years of painful electrolysis to get rid of facial and body hair and surgery to reconstruct her breasts.
Now married to a "wonderful" man, Angela has three young children and has slowly rebuilt her life. Looking back, she acknowledges she gave consent for the procedure but believes it was not informed consent. She feels she was mentally ill and that her childhood abuse played a part in her gender confusion.
Below are several anecdotal examples circulated on social media that seem to validate trauma’s influence on gender dysphoria in some cases.


E. Anti-homosexual attitudes
Detransitioned lesbian (1:35-1:53), (:32-:45):
This was the year 2006 and at this time it was incredibly rare for anyone below the age of about 23, a female to start medically transition
Everywhere I go now in all LGBT meetings I would say about 80% of ones who probably would’ve called themselves lesbians are calling themselves trans and transitioning. And I think there must be questions
The subject matter of this website pertains to the environment children, teens, and young adults are exposed to, who have not reached full maturity, and look to the surrounding culture to form their identities, according to developmental psychology research. Although more heterosexual biological females are transitioning, a large portion of those medically transitioning are same-sex attracted young females.
There are multiple examples of transitioning being related to internal and external anti-lesbian feelings, which do not appear to be positive reasons for undergoing hormone therapy and surgery. This study confirms that homophobic bullying can push a youth towards trans identification and we discuss anti-homosexuality influences in this section and here. There is not one “LGBT” website or “LGBT” organization that will even dare to raise any concerns over this issue for fear of accusations of transphobia. Funding for “LGBT” organizations is largely coming from trans activism. The general apathy and desire to hide the realities of the struggles young lesbians, and increasingly bisexuals, and how homophobia appears to encourage them to identify as trans will likely continue.
Young lesbians used to be able to find whole support groups with peers and community, at least in urban areas. That has changed.
Our lesbian daughter is the only non-trans person in her entire GLBT youth group. Now who is she going to date?
Here is a statement by a detransitioned lesbian:
The only time I was exposed to butches at all was when they were the butt of jokes on television. People used the term butch to describe me when they were insulting me. Butch was what happened when girls didn’t grow out of being tomboys like they were supposed to.
A parent’s (blog censored by Wordpress) comment about their previously lesbian identified daughter:
Last year’ she was ok with being lesbian. This year she told me “ew that’s gross!! That’s not me!”
An FtM had a very bad experience living as a lesbian:
That term, just before summer break, Alex realised she was attracted to her female best friend: “And I ended up, stupidly, telling people at school that we were in a relationship. I didn’t think I was a lesbian or anything like that. I just thought, ‘This is somebody that I’m really into. Why can’t we be together if we have a connection in a similar way that I would if I found a boy that I liked?’ ”
In September, starting at a huge new secondary school, Alex and her girlfriend found themselves surrounded by a jeering gang. News had spread. Alex felt panicked, anxious. She hadn’t even told her parents. “I was known as the ‘weird lesbian girl’ and nobody would speak to me, and suddenly it was just really hard, because I’d never found it difficult to make friends really.” She’d go over to her old mates, the video-game boys, but they’d walk away. “My sexuality tainted their perception of me entirely.” Among the post-pubescent “masculine” boys and “feminine” girls she was an oddity: a masculine girl. “I was the misshapen cookie, the one made at the end with the leftover dough that gets burnt and no one wants to eat that.”
Despite having medically transitioned and saying that was the right decision, Alex Bertie still hates looking at an unclothed body in the bathtub in that article.
For some reason FtMs like Alex Bertie, Chase Ross, and other young FtMs are treated as celebrities in a way no young lesbian ever was, even at the height of gay and lesbian rights activism. One desister lesbian notes this pattern as she was showered with attention after coming out as trans:
To exactly nobody’s surprise, Tumblr was ecstatic at my ‘realization’. A plethora of congratulations, encouragement, and support was sent my way–something that girl-me never got for being exactly the same as boy-me, save having a different name and pronouns.
Here is another example of a doctor observing the reality that “trans boys” are much more supported and popular than lesbian youth and that they have a lot more power.
A woman I will call Dr K expresses years of frustration dealing with an unacknowledged epidemic of dysphoric teenage girls. “They are all the same, dozens and dozens of them. Short hair, boys’ clothes, probably liked rough and tumble play as small children. Now they like comic books or skateboarding or video gaming. Geeky, gauche, not many friends. They came out as lesbians, but then they went on Reddit and Tumblr and saw these transitioning videos. They decide they are trans. Suddenly they get lots of attention with everyone calling them by a new name, they get to chide anyone who uses the wrong pronoun while everyone tells them they are brave. They might get a special assembly at school.”
In the same London Times article an FtM support group leader is even alarmed at the pro-medical transition culture among lesbian youth:
Peter lived as a woman until his late forties when, after extensive therapy, he became a trans man. “I just knew I had to do this to be happy. I was simply not a woman.” He now runs a trans support group and is aghast at an online culture pushing young lesbians into hasty transition. “I think some of them actually want done to hold on to the transitional state. For a girl who was once marginalised, it has prestige. You post videos updating your progress. You get endless attention.” But actually living in your new gender can be a letdown. “They find their old pr dooblems have not gone away. And we pick up the pieces.” Peter knows trans boys w` stop with the fact who that fucking hate thatho consulted private doctors to obtain hormones without prior counselling “and now they’ve had a breakdown and are asking Facebook friends to donate money for therapy they should have had first.”
From a blog post, “It’s better to be a cute boy than an ugly butch lesbian”:
As time passed, I started to feel ashamed about being a lesbian within the queer community. As one ex said to me “lesbianism is sooooo last century”. I was butch too, a real stereotype. I was ashamed of being a butch lesbian stereotype, and felt that I sucked at being a woman so much, that maybe I couldn’t be one, but the term “genderqueer” left me cold. I also didn’t fancy men, and they didn’t fancy me.
A detransitioned male who has also counseled “queer” youth is worried for lesbian young people:
At the queer counseling center I worked at, one of the directors told me that there was a 400% increase in transgender clients in the last few years. I believe this is because the queer cultural explanation of cross-gender feelings has changed. Rather than people saying “you must be gay/lesbian” they say “you must be trans”. I see disturbing parallels between “lesbian until graduation” which was a common idea when I was in college, and the explosion of young people identifying with the FTM-spectrum identities. The difference is that “lesbian until graduation” can be an adventurous time in college, while “trans until graduation” has permanent severe consequences as changes cannot be completely undone.
There are many accounts from lesbians that talk about anti-lesbian and anti-butch attitudes that are internalized in the LGB and T populations themselves, and in the society at large. Here is a question and answer on a detransitioner’s blog called redressalert.
Anonymous asked: do you have any advice on dealing with homophobia from lesbians? Many have a strong problem with "butches" and don't want them to exist as part of the community.
Someone told me the reason i had a problem with my sexuality is because i'm "butch"; that butches are the reason why homophobes hate gay people, and if i were feminine, i wouldn't have a problem. it's so common, always comes with an intense, spiteful attitude as if i have done something wrong and confirms my deep feelings of alienation
I’m sorry you’re dealing with that. It’s hard when it comes from other lesbians. Lesbians on the whole have typically been seen as a type of “female man” or as having something suspect about our womanhood, regardless of how we look. Lesbians internalize that in different ways. Some think, “I must really be a man inside,” and others (unconsciously or not) try to defy that expectation in every way possible, sort of to “compensate” for being with women by proving how acceptably “womanly” they are in every other way. If you have other lesbians blaming you for being mistreated by the straight world, that’s classic victim-blaming. “Stop making us look bad, we’re trying to prove we’re Just Like Them”–that’s never ultimately been a workable solution for lesbians. If they’re taking stuff out on you, that is not your fault. It’s not your fault that being an overt dyke means a lot of society comes down hard on you. So I think they have their own stuff they need to work out. But homophobia comes from misogyny, its use is in maintaining men’s control over women. So there’s a lot of threat when you are a woman who won’t mark herself submissive to that order, who in fact openly defies it. A lot of women are not prepared to openly defy it, and a lot of women blame other women for what men do as a matter of course.Horizontal hostility is a real thing. I recommend finding other butch dykes, and out, overt dykes in general who will get what you are going through. Talk to them about your feelings. You’re not alone.
This an anonymous comment on a social media page:
An anonymous comment:

Another comment from a dysphoric lesbian:
I am sad for these young people, not so much because they are behaving badly (although they are, but teenagers make bad decisions when pressured by peers and powerful ideologies like trans discourse), but because i am sad for my former self. i do not know how to be a lesbian, or a GNC woman. i am still dysphoric. i am still struggling with liking women. the places where i could have gone, as a teenager, to learn about those things, the places where lesbians were, older women who could have mentored me, those places are largely gone. now queer spaces are filled with people like my younger self– angry, hurt, afraid, confused, and unwilling to listen.
She also discusses how lack of representation and anti-lesbian hatred affected her:
i discovered detransitioning blogs on tumblr and realized that, as a child, no one ever presented being a GNC female as an option to me. i was not feminine. i liked girls. i did not want to be a lesbian. i didn’t know any lesbians personally and like every other young girl in the US i grew up thinking that dykes were fat and ugly and aggressive and smelly and no one liked them. it was inconceivable to me that i could be a happy lesbian, much less a happy, non-feminine woman. it was inconceivable to me that i could deal with my dysphoria (my hatred of my body but especially my hatred of how men treated my body, and how society treated me because of my body) in a way that did not involve altering or obliterating it.
Seeing lesbian representation seems to help some young lesbians with their gender dysphoria.
Jessie’s friends had started to bind their breasts: some strapped so tight, they threw up. She tried, but it made her out of breath. Then her mum found her binder and threw it away.
Over a turbulent 18 months, the feeling she was a boy gradually faded. Why? She got a girlfriend and saw her transitioning friends were still deeply troubled. “But the biggest factor was that I moved from music stuff to TV fandom.” She watched Supergirl, which has two lesbian characters, Maggie and Alex, a secret agent and a cop; and Wynonna Earp, with action lesbians Waverly and Nicole who fight demons. “It sounds mad, but they changed my life: finally I saw girls I wanted to be.”
Now Jessie is 17, starting A levels, a happy, sociable, “out” lesbian. “I don’t see why there should be a male box and a female box. Just people who happen to have a penis or a vagina.”
What would have happened if her mother had taken her to a gender clinic? “I would have been Jake now. No question. But I wouldn’t have been happier at all.”
Transgendertrend, website in Britain following the trend of a spike in trans identified young people, also indicates lesbian support can help some dysphoric youth.
There is no acknowledgement or support for these young lesbians in schools and no funded youth groups for them outside of school, although there are manyfunded trans youth groups. We have been in contact with some of these young lesbians, who have told us about the pressures on them to define as men and who would have transitioned if they had not found lesbian feminist groups. We have also been contacted by female detransitioners who now define as lesbian. They deeply regret the harm to their bodies inflicted by sex hormones and having double mastectomies. They question how they were allowed to receive this medical treatment so young. They tell us if they had been supported in school or by lesbian youth groups they would never have transitioned.
An older lesbian helps a younger lesbian work through gender dysphoria:

There are multiple cases of lesbians/bisexual/heterosexual females desisting on 4thwavenow.com, a website for parents skeptical of medically transitioning minors and young adults, here, here, here, here, here, here, and here. What is disturbing about these stories is that these teenage girls all met the criteria of “persistent, insistent, and consistent” for at least six months, to justify medical interventions (hormone blockers, cross-sex hormones and now even surgeries) that are being performed on teenage girls as young as thirteen in the US. Then they grew out of it, even after several years of insisting they were trans, insisting on hormones, and insisting on top surgery.
These stories strongly indicate that the affirmation model will transition teenagers who would have resolved their gender issues if there weren’t gender clinics, as has been shown by research. Enthusiastically medically transitioning even late onset cases, with no mental health screening as it is considered conversion therapy, is certain to create false positives and already has. It will only be a matter of how many. In many of these stories the therapists and doctors were extremely supportive of medically transitioning these young people immediately.
Doctors are not even considering the possibility that gender nonconforming females could live as lesbians. This screen cap is a comment circulated on Twitter, from a parent of a young person, who would have met DSM-V criteria for medical transition at a gender clinic:

There are many older lesbians who are very disturbed by new protocols to medically transition minors and society’s enthusiasm around it. Camille Paglia is both a feminist and critic of feminism, a cultural critic, a professor, and a writer who has this to say:
Beyond that, I believe that my art-based theory of "sexual personae" is far more expansive and truthful about human psychology than is current campus ideology: who we are or want to be exceeds mere gender, because every experimental persona that we devise contains elements of gesture, dress, and attitude rich with historical and cultural associations. (For Halloween in childhood, for example, I defiantly dressed as Robin Hood, a Roman soldier, a matador, Napoleon, and Hamlet.) Because of my own personal odyssey, I am horrified by the escalating prescription of puberty-blockers to children with gender dysphoria like my own: I consider this practice to be a criminal violation of human rights. Have the adults gone mad? Children are now being callously used for fashionable medical experiments with unknown long-term results.
Here is another anonymous example from social media of an older lesbian who feels this could have been harmful to her as a youth:

With the increase of teenagers and young adults transitioning, there is certain to be more cases like the ones below.


{kind=link}
And this lesbian who detransitioned at age 22.
James Caspian is a gay man who is a therapist who has worked with trans patients. He is very concerned about the mounting numbers of regretters. Bath Spa University refused to allow him to do any research on detransition because it would anger trans activists. There is more on the topic of censorship here.
And in that 2 years, I was constantly uncovering more and more, particularly young women who were regretting transition. And I was reading what they were saying, that they been kind of caught up in something, it was kind of a bit of a movement, amongst particularly young lesbians it seemed, to move into the whole idea of being trans. And the whole idea of being trans which as un umbrella term had become huge and vast… and almost cover everybody.
F. Female autism
This section contains citations and discussion about the links between autism and gender dysphoria in both sexes. It is worth watching the entire video below by CaseyJeanC, a re-identified woman on the autism spectrum, to understand trans identification in females with autism. She covers topics such as sensory processing issues, difficulty with gender roles, social awkwardness, and the allure of a framework and being part of a supportive group when you are autistic.
Tania Marshall has had both gender dysphoric and autistic female clients. Below is a description of some of these individuals.
A lot of the girls have reported to me not fitting in with girls. They are seen as quirky or eccentric tomboys. They report being bullied or being told that they are a boy. That they look like a boy. And this makes them feel that they must be a boy. They have reported not being allowed to play boys games with the boys and so they get really confused. Another factor that I think is pretty big is society and the culture is male privilege. This has come up time and time again. So, I’ve got intellectual, very intelligent talented females talking about male privilege. “Males are paid more. I wouldn’t be treated like that if I was a male. I’m treated as if I know what I’m talking about. I don’t have to apologize. Guys like hanging out with me. I didn’t think I had privilege, now I have more equity. I make more money and I have more opportunities.” This is from my male client. Now male (FTM). And he said “I remember my dad and how he would play with his cousins. And I really wanted that. And I realized that I saw my dad have social status. And I wanted to avoid a lifetime of sexism.
Autistic teenagers searching for a reason why they have not been able to fit in will fixate on the idea that they were born in the wrong body. I have seen this time and time again. With males and females. These females are often late diagnosed or often don’t have a diagnosis at all. Or are misdiagnosed. All or nothing black and white thinking is a contributor. The individuals lack the capacity to see other answers, explanations or reasons. Some of them come out as lesbians, have mild autism, and mild to severe mental health issues. They have all been adolescent girls.
She also provides many examples of females being bullied by other females for not being sufficiently feminine.
Below are examples of bisexual females on the autism spectrum who feel being emerged in a pro-medical transition culture could have harmed them. It appears GD and lesbianism/bisexuality, are associated with autism spectrum females and more of these women are speaking out in media and social media.
One client said she only came out as a lesbian in college because she came from a very authoritarian religious background that was very rule bound, very black and white and took things very literally, took the Bible literally. So, she didn’t come out until college. She came out as bisexual. And then she said to me that she was glad she was not teen in 2018 today because she said, “If I were that age today I could totally see myself as identifying as transgender when I am not. So, there’s quite a few clients who are older who are reporting to me that they do see that they do understand that the younger generation of today of 2018 would but come to the belief that they are trans. But then she said it was a couple of years later she realized that she not, she was just a lesbian. And she was very very glad that she had not proceeded with taking hormones and transitioning. So, this is telling me this is a phase.
A bisexual woman, on the autism spectrum from a religious background, expresses similar concerns over the diagnosis of same-sex attracted autistic young people being enthusiastically affirmed.
More and more frequently, I read about autistic youth being diagnosed as transgender. As a bisexual woman, it’s a double whammy to see how many LGB youth are being encouraged to transition, and to share the concern of other LGB adults who read the transition stories of young people, even small children, and find ourselves thinking that this could have been our own story. These concerns are almost frantically brushed aside with claims about suicide risk that don’t stand up to scrutiny.
To be clear, I’m not talking about people who had full, successful lives as heterosexual males, with families and distinguished careers behind them, before they drastically upended their lives. Their experiences are as if from another world. But when I read stories about kids — especially girls — who had childhood crushes on the “wrong” people, played with the “wrong” toys, or felt awkward all the time and were isolated because they couldn’t compensate, I relate. And I worry.
G. Conclusion, why are there so many females?
Given that:
there is such a large increase in gender dysphoric female tweens, teens, and young adults that doesn’t match previous adult ratios
there is much historical evidence for socially contagious self-harming, body dissatisfaction, and mental illness, especially in females
there are teenagers identifying as trans and growing out of it at risk for irreversible effects of testosterone and double mastectomy
abuse appears to influence a young female to want to transition
previous data showing low regret rates were mostly done on adult transitioners who transitioned a more cautious model, even for adults
regret rates among young females appear to be increasing
there is evidence anti-lesbian/bisexual attitudes fuel gender dysphoria and transition
there are often many comorbid conditions
adults are responsible for the wellbeing of children and teenagers
…it is incumbent of therapists and doctors to consider all of these factors in treating youth with gender dysphoria. Highlighting these issues also demonstrates the problem with anti-conversion therapy laws, that may prevent exploration of these factors. There are some young people who have other issues around mental illness, trauma, internalized homophobia that are reinforcing their gender dysphoria in the current social environment. This could cause misdiagnoses, with physical consequences for the teenage girl and perhaps legal consequences for adult mental health and medical professionals.
Thirdwaytrans advocates for better approaches and research to discern who is best served by transition and who may be motivated by other factors that may cause them harm if they transition.
Again just as the existence of “lesbian until graduation” does not deny the existence of those who retain a long-term lesbian identity that is healthy for them, neither does the existence of “trans until graduation” deny the existence of those for who testosterone use and male presentation is right. The difference is that it is important to find better ways to distinguish between the two before people take T if possible. How to do this? I don’t know, but I suspect looking at misogyny, gender schemas, dissociation and trauma is a good place to start.
© Gender Health Query, 6/1/2019
For updated information regarding topic 11
REFERENCES FOR TOPIC 11
Continue to Topic 12:
Contents
11) Why are so many females coming out as trans / nonbinary?
A. Evidence for large increases in females identifying as trans
-Affirmative model advocates’ explanations for increasing numbers of trans identified females
G. Conclusion, why are there so many females?
Back to Outline
MORE
1. Do children outgrow gender dysphoria?
3. Are children & teens old enough to give consent?
4. Comments safety / desistance unknown
5. Gender dysphoria affirmative model
6. Minors transitioned without any psychological assessments
8. Regret rates & long term mental health
13. Why is gender ideology being prioritized in educational settings?
14. Problems with a politicized climate (censorship, etc)