ORIGINAL TOPIC POST= 2) CONSEQUENCES & PERMANENT SIDE-EFFECTS THAT RESULT FROM THE USE OF HORMONE BLOCKERS
We are updating our Topics in 2023 with the most recent and relevant information regarding over-medicalized youth and identity confusion due to queer theory/gender ideology. Since the launch of our website in 2019, only more information has come to light validating our view that pediatric transition is dangerous for children and teens. We support honest and open inquiries regarding this topic. Our focus is protecting lesbian, gay, and bisexual youth from harm, and we want the best long-term health outcomes for all youth, regardless of identity or orientation.
More serious health consequences from puberty blockers, cross-sex hormones, and surgeries are coming to light. This information is forcing the trans-activist-captured legacy media to admit there is anything dangerous about the affirmative model protocol.
They Paused Puberty, but Is There a Cost? As more transgender children seek medical care, families confront many unknowns
We are adding a study indicating the pubertal process is very complex regarding brain maturation.
Coming of age in the frontal cortex: The role of puberty in cortical maturation (Delevich et al., 2021)
Medical Ethics
Due to increasing evidence of harm, several republican dominated states are banning pediatric transition. These laws will be challenged, and this will be a legal battle in the United States for a long time. Health Query does not involve itself in legal battles currently. But we believe it is better for medical ethics board reviews to curtail pediatric transition rather than legislatures. Or, in this case, where the state is merely enforcing existing laws.-
https://twitter.com/agandrewbailey/status/1637882764706848773?s=46&t=_nlFr-A1tHVIfNQH-_MaeA
https://threadreaderapp.com/thread/1637882764706848773.html
Given institutions are caving to activist pressure in the internet age; this is not going to happen at the higher levels or in liberal states anytime soon. Liberal states are making themselves "sanctuary states" for “gender affirmative care,” for runaways, parents who want to medicalize their child, or parents in custody disputes.
Sweden, Finland, the UK, and Norway are countries that are now revieing evidence or curtailing the practice.
Damage From Puberty Blockers
Articles about the dangers of giving puberty blockers to kids-
”New report describes dangers of giving Lupron to kids”
“Use of Gonadotropin-Releasing Hormone Analogs in Children: Update by an International Consortium ‘My body is on fire’: Ga. woman blames drug for pain, sues maker” (Krishna et al., 2019):
Lupron was originally Food and Drug Administration (FDA) approved to treat prostate cancer, but it’s now routinely prescribed for other conditions such as endometriosis and “precocious puberty” — i.e., puberty that begins too early (generally considered under age eight for girls, under age nine for boys). Many of these patients have experienced extreme side effects that shattered their health and their lives, including severe joint pain, osteoporosis, compromised immune systems, and mental health issues such as severe depression and even suicidal ideation. The FDA has received 24,000 reports of adverse reactions, about half of which the agency has deemed serious.
”More women come forward with complaints about Lupron side effects” (suicidal thoughts as a side effect which may be of concern when given to troubled tweens and teens)
Conclusive evidence transitioning male tweens permanently destroys their sexual function
Doctors have permanently destroyed the sexual function of all or most males they puberty-blocked in Tanner stage 2. They will likely experience permanent anorgasmia. Below are WPATH members admitting to this. This is likely due to both the child-like state of the genitalia and the impacts on brain wiring when doctors severely interfere with the pubertal process. Marcie Bowers, a trans-identified heterosexual male, is a vaginoplasty surgeon. Bowers performs experimental and complicated surgeries on minors. The surgery is difficult due to the genital stunting induced by the puberty blockers.
https://twitter.com/DonovanCleckley/status/1521625518394773505?s=20:
Every single child, or adolescent, who was truly blocked at Tanner stage 2 [by age 11] has never experienced orgasm. I mean, it’s really about zero.
Jazz Jennings was a victim of this effect and a botched vaginoplasty that needed 3 revision surgeries. Bower’s admits in the video that this is detrimental to relationships due to Bower’s experience in dealing with victims of female genital mutilation:
The lack of being able to be intimate with a partner is very important.
This is the sexual lobotomization of children at a stage where they are pre-sexual. Gender Health Query believes this is a human rights crime. Children cannot consent to permanently destroyed sexual function before any sexual experiences. There are no serious calls among “affirmative model” advocates to delay puberty blockers to preserve sexual function, only prescriptions for parents to tell their 10-13 year olds to “masturbate more” before the chemical castration process begins, if even that.
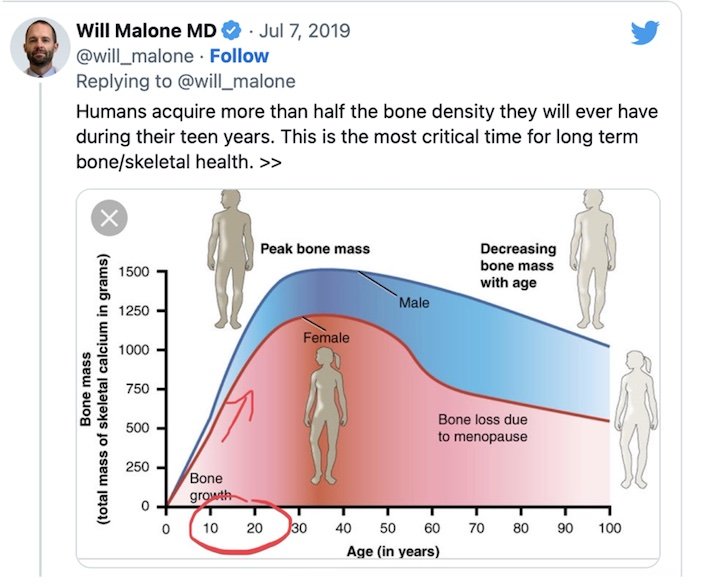
More proof of bone density loss
Major bone mass accrual happens in puberty and then is lost as we age. The problems of reducing bone mass accrual in puberty is obvious.
Endocrinologist Will Malone:
Jesse Singal posted an interview with Swedish journalist Carolina Jemsby, who has been reporting on the negative fallout from pediatric medical transition in her country and Karolinska hospital specifically. Sweden is curtailing pediatric transition due to damage resulting from it. The journalist states one 15 yr old has such a severely damaged spine the youth can’t stand up for more than 20 minutes without pain. The journalist said there were other recorded injuries from using hormone blockers and that the doctors seemed very motivated to avoid tracking harm and taking it seriously.
Other articles indicating bone loss due to puberty blockers-
”Pubertal Suppression, Bone Mass, and Body Composition in Youth With Gender Dysphoria” (Navabi et al., 2021)
”Revisiting the effect of GnRH analogue treatment on bone mineral density in young adolescents with gender dysphoria” (Biggs, 2021)
”Hormone Agonist Therapy Disrupts Bone Density in Transgender Youth”
”Puberty blockers for gender dysphoria: the science is far from settled” (Malone et al., 2021):
The Karolinska Institute in Sweden, long considered gold-standard in providing transgender health care, no longer uses puberty blockers;6 nor does Finland promote their use.7 Additionally, a judicial review in the UK found puberty blockers to be an inappropriate option for most children younger than 16 years. 8 We urge The Lancet Child & Adolescent Health to take this opportunity to engage with this issue, rather than publishing, in our opinion, inaccurate and careless Editorials.
”Puberty blockers revealed to be dangerous for minors: study”
”Puberty blockers ‘stunt bone growth of children”’
We cannot verify the validity of the statements on the r/detrans subreddit below. But it provides insight into how this may be impacting young people in the real world.
https://www.reddit.com/r/detrans/comments/mbmm7x/lupron_side_effects/:
Brain bleeds and vision loss
”FDA Updates Safety Labels for Group of GnRH Agonists”:
Some children who have received GnRH therapies have experienced pseudotumor cerebri, which results in elevated spinal fluid pressure in the brain. This can lead to progressive loss of vision.
Puberty blockers use my increase the likelihood of depression
”Puberty blockers do not alleviate negative thoughts in children with gender dysphoria, finds study” (Dyer, 2021)
The Daily Wire is a conservative website that holds anti-LGB views we oppose, but author Christina Buttons is not of those opinions. We must cite these sources due to the widespread denialism that there are severe dangers to the “affirmative model” in legacy media.
The results found that treatment with leuprolide, the drug used to suppress puberty, had “profound effects” of increased depression in female mice; in male mice, increased stress and a loss of interest in female mice were reported.
From the study ”Behavioral and neurobiological effects of GnRH agonist treatment in mice-potential implications for puberty suppression in transgender individuals” (Anacker et al., 2021):
Our behavioral and neurobiological characterization reveals for the first time that chronic leuprolide treatment, starting after the onset of puberty, exerts sex-specific effects on social preference, despair-like behavior and hyponeophagia, neuroendocrine responses to mild stress, and hyperactivity of the [dentate gyrus], a crucial neurobiological regulator of stress responses in mice.
And:
In conclusion, we report that chronic leuprolide treatment in mice has profound effects on female behaviors that are commonly interpreted as depression-like, as well as on neural activity in the hippocampus—a brain region crucially involved in stress processing, depression, and cognition,” the discussion section read.
While these mood-related effects are specific to females, leuprolide causes pronounced differences in locomotion and social preference in males and increases neuroendocrine responses to mild stress,” the researchers added.
Back to the Daily Wire news article (emphasis ours):
Dr. Claudia Gennari, an internist and researcher, believes the negative psychiatric outcomes found in this study have huge implications for pediatric gender medicine.
This study was long overdue and should bring pause to clinicians treating children with puberty blockers because it shows sex-specific neuropsychological changes caused by this medication,” Gennari told The Daily Wire.
This strongly suggests GnRH agonists are not a ‘pause’ button at all and its use can cause negative effects on cognition, behavior, and coping skills,” she added.
Puberty blockers likely increases persistence
Affirmative model advocates have effectively promoted the “true trans” narrative and social and medical transition as healthy and safe to the public because they are heavily invested in the protocol they encourage. For example, one can find very ideological language written in the Dutch study below, indicating most children/teens who go on puberty blockers persist and go on to transition.
”Continuation of gender-affirming hormones in transgender people starting puberty suppression in adolescence: a cohort study in the Netherlands” (van Der Loos et al., 2022) (emphasis ours):
Most participants who started gender-affirming hormones in adolescence continued this treatment into adulthood. The continuation of treatment is reassuring considering the worries that people who started treatment in adolescence might discontinue gender-affirming treatment.
There is no reason to state this is reassuring. The only way to glean the effects of social and medical transition on minors would be to have a control group of youth who are loved and supported but aided in getting through a healthy puberty and, perhaps, young adulthood until maturation at age 25. It is logical to consider that adding chemicals that strongly affect the brains of growing adolescents may affect their identity development and choices. Stating it is “reassuring” almost all go on to transition is purely ideological on their part and inappropriate for science researchers.
This translates to biased reporting in the media and a propagandized public. Journalists rarely asks why almost all kids are going on to transition. This is the case with the NPR article ”Most teens who start puberty suppression continue gender- affirming care, study finds,” a source that should be unbiased. This enables apathy about what appears to be increasing persistence.
This part of the study indicates transitioning minors increases persistence. Or it may mean they were more dysphoric from childhood, and those who “come out” later are at more risk of regret:
People who started hormones as minors had higher continuation rate than people who started as adults 74.4% (66.0%-82.8%) vs 64.4% (56.0%-72.8%).
In this study the females were likelier to abandon hormone treatment than the males, concerning given the explosion in trans identity in females:
Transfeminine individuals had a higher continuation rate than transmasculine individuals 81.0% (72.0%-90.0%) vs 64.4% (56.0%-72.8%).
Case reports of desistance post puberty blockers
This is a relevant thread on the r/detrans Subreddit. Several of the young people desisted or detransitioned after the use of puberty blockers.
Has anyone here been put on puberty blockers? How has that affected you?:
yes, i was on lupron and testosterone for 11 months starting from the month after i turned 14 to right as i was turning 15. my breasts definitely shrunk a lot (below an a cup) but generally returned slowly, although they never were that big to begin with. i’m now almost 16 and i got my period six and a half months after i started detransitioning. in my opinion blockers shouldn’t be used on minors (in gender transition cases.) another note, the endo that prescribed me lupron did a ‘puberty test’ (i believe it’s the tanner scale test?) except rather than just peeking at my clit development, she squeezed and poked my nipples and stared at my clit with nobody else in the room. this was meant to be preparation for puberty blockers but having read up on this procedure afterwards she definitely was going against the rules of it. on the bright side, i did make it out alive and i am doing generally okay now, at least much better than i was. i think that puberty blockers (or t, or a combination) caused me severe dissociation during the time i was taking them as i had very little coherent thought, i feel as if once i started them i just kind of checked out in terms of life. once i went off both my sense of self returned and i have a level head. :)
The evidence for puberty blockers reducing suicide risk is weak to nonexistent.
Despite a strong drive to promote “affirmative care,” and thus puberty blockers, as “lifesaving,” the evidence for this claim is not strong.
”Puberty Blockers and Suicidality in Adolescents Suffering from Gender Dysphoria” (Biggs, 2020):
A report regarding GIDS Early Intervention Study (beginning in 2011) found there was no overall improvement in mood or psychological wellbeing using standardized psychological measures
Tavistock’s Experimentation with Puberty Blockers: Scrutinizing the Evidence
Reasons not to sexually lobotomize and sterilize youth
As we have pointed out in the original Topic #2 article, many trans people want sex lives and to have children.
In the Heterodorx podcast by Nina Paley and trans-identified Corinna Cohn, they talk about the sexual orientation of GAMP. Corrina states that males who want to be females who don’t get bottom surgery are in much higher demand than those who have had it. While there is an unfortunate amount of exploitation of trans people by “chasers,” we believe that males who have this sexual orientation, best described as a type of bisexuality, should facilitate healthier relationships with feminine males with less drastic, expensive, and health-damaging surgeries. Minors cannot weigh the cost of “passing better” to invasive and health-damaging and sexuality-damaging medical procedures.
Episode 42: GAMPs, Pr0n, trans, and the Conservation of Evil
There are more stories of lawsuits from people angry they are now sterilized as a requirement for transition proving fertility is of great importance to many. The same thing is happening in Sweden.
”Transgender Germans seek compensation after forced sterilisation”
Random PB studies
We consider the below study to be poor quality.
”Review: Puberty blockers for transgender and gender diverse youth—a critical review of the literature” (Rew et al., 2020)
We have demonstrated there is weak evidence for the “lifesaving care” claim they make in they make in their conclusion. They also include Jack Turban, who does poor quality research. One study has one participant. And they do not clearly state their search criteria.
The below study on delayed puberty due to congenital hypogonadotropic hypogonadism (Kallmann syndrome) may provide some insights into side effects from delaying puberty in youth.
”Psychosexual effects resulting from delayed, incomplete, or absent puberty” (Dwyer, 2020)
Conflicts of interest in puberty blocker studies
From an article in The Post Millennial, ”Maker of puberty blockers funded original study that led to 'gender-affirming care' for minors: Dutch investigative report”:
A Dutch investigative report has revealed that the 2006 study upon which the entire medical experiment of child sex changes is based was funded by a maker of puberty blockers.
The NRC article, published on Dec 31, takes aim at the treatment approach known as the "Dutch protocol," which involves blocking the puberty of adolescents who are suffering from gender dysphoria and forms the basis for the "gender-affirming care" model adopted by pediatric gender clinics all over the world.
”Ook transzorg moet aan medisch-wetenschappelijke standaarden voldoen”
Another article on Ferring Pharmaceuticals’ involvement in Transgendertrend-
“‘They Look Normal’ – The Case For Puberty Blockers”:
I would want to know why a drug company, Ferring, sponsored the crucial Dutch trial into puberty blockers: the 2006 Delemarre-van de Waal and Cohen-Kettenis paper was ‘presented at the 4th Ferring Pharmaceuticals International Paediatric Endocrinology Symposium, Paris (2006)’ and Ferring Pharmaceuticals supported the publication of these proceedings.’
”Short-term outcomes of pubertal suppression in a selected cohort of 12 to 15 year old young people with persistent gender dysphoria in the UK” (Carmichael et al., 2021) Almost all youth put on blockers persisted and went onto cross-sex hormones and there seemed to be no psychological improvements:
Treatment of young people with persistent and severe GD aged 12–15 years with GnRHa was efficacious in suppressing pubertal progression. Anticipated effects of withdrawal of sex hormones on symptoms were common and there were no unexpected adverse events. BMD increased with treatment in the lumbar spine and was stable at the hip, and BMD z-score fell consistent with delay of puberty. Overall participant experience of changes on GnRHa treatment was positive. We identified no changes in psychological function, quality of life or degree of gender dysphoria.
”Thrombosis Risk in Transgender Adolescents Receiving Gender-Affirming Hormone Therapy” (Mullins, 2021)
This study has a very short window of time, so is not particularly relevant for health effects. There are also conflicts of interest because it’s funded by the makers of puberty blocker Leuprorelin.
Sex Hormone effects
Brain effects
While issues such as depression affect cognitive health, the bad news about brain health in trans individuals is likely due to taking large doses of cross-sex hormones, yet they seem unwilling to focus on this question in the below article.
”’Alarming' Data on Early Cognitive Decline in Transgender Adults”
Cross-sex hormones affect the brain structure of males and females. Adults may be desirous of these changes, but adolescents' brains are not fully formed, nor is their understanding of themselves.
”Cross-sex hormones alter grey matter structures” (Holmes, 2016):
Analysis of brain structures revealed volume changes predominantly in MtF individuals, particularly in the hippocampus — a region involved in neurogenesis and neuronal plasticity. Specifically, oestradiol plus anti-androgen treatment reduced hippocampal volume in MtF individuals, which was accompanied by a global increase in ventricular structures. Moreover, reduced plasma levels of progesterone in MtF individuals correlated with reductions in grey matter structures in the right hippocampus and right caudate. "These structural changes are associated with aging and Alzheimer's does this and so does estrogen...
Fertility effects
Fertility concerns of the transgender patient (Cheng et al., 2019)
Testosterone therapy in transgender men can suppress ovulation and alter ovarian histology, while estrogen therapy in transgender women can lead to impaired spermatogenesis and testicular atrophy.
Bone effects
The below study review study ran into major problems due to lack of consistency in study designs but did find trans-identified males may have lower bone mineral density.
”Systematic Review of the Long-Term Effects of Transgender Hormone Therapy on Bone Markers and Bone Mineral Density and Their Potential Effects in Implant Therapy” (Delgado-Ruiz et al., 2019)
A review indicating dysphoric people do want children-
”Desire for children and fertility preservation in transgender and gender-diverse people: A systematic review” (Stolk et al., 2023):
The majority of TGD people expressed a desire for children. Fertility preservation utilization rates were low as there are many barriers to pursue fertility preservation.
Circulatory effects-both sexes
”Hormone therapy for gender dysphoria may raise cardiovascular risks”
”Cardiovascular Disease Risk Factors and Myocardial Infarction in the Transgender Population” (Alzahrani et al., 2019):
Conclusions: The transgender population had a higher reported history of myocardial infarction in comparison to the cisgender population, except for transgender women compared with cisgender men, even after adjusting for cardiovascular risk factors.
”Hormone therapy for gender dysphoria may raise cardiovascular risks”
”Assessing and Addressing Cardiovascular Health in People Who Are Transgender and Gender Diverse”
In addition, the use of gender-affirming hormone therapy may be associated with cardiometabolic changes, but health research in this area remains limited and, at times, contradictory.
The study below shows a decrease in blood pressure for trans-identified males but an increase for trans-identified females.
”Blood Pressure Effects of Gender-Affirming Hormone Therapy in Transgender and Gender-Diverse Adults” (Banks et al., 2021)
Estrogen specific effects
This post is from a parent of a trans-identified person and not a medical review. But it contains some valuable and in depth information in greater detail than covered here.-
Most transgender care providers will mention venous thromboembolism or VTE as the predominant risk from estrogen, but research in the past few years indicates that its effect on the brain is at least as scary.
Giving male tweens and teens puberty blockers and estrogen likely has significant influences on their brain development, including brain volume shrinkage in some areas.
Effects of adult male rat feminization treatments on brain morphology and metabolomic profile (Gómez et al., 2020):
These results reveal, for the first time to our knowledge, that the volumetric decreases observed in trans women under cross-sex hormone treatment can be reproduced in a rat model. Estrogens are more potent drivers of brain changes in male rats than anti-androgen treatment.
The study ”Psychosocial Functioning in Transgender Youth after 2 Years of Hormones” (Chen et al., 2023) showed some improvement with HRT for females, but not males. We fear estrogen in males may be associated with depression.-
“Increased estrogen level can be associated with depression in males” (Stanikova, et al., 2018)
Posting relevant quotes from ”Health considerations for transgender women and remaining unknowns: a narrative review” (Iwamoto et al., 2019)-
Some dysphoric people will obtain hormones from black market sources. Attempts to outright ban this practice for adults will fuel this phenomenon:
When barriers prevent trans people from obtaining GAHT from a licensed medical provider, they may search for other sources. Previous reports stated that 4.7–24% of TW have obtained hormones from friends,44–46 and 2–70% have purchased them online.47 Anecdotally, some TW who utilize services at the Ghent University Hospital Transgender Infopunt have admitted to using OCPs obtained from their female partners. The use of GAHT obtained from nonmedical sources varies from 23% in a United Kingdom sample of trans people referred to a gender clinic,47 to 26.8% in a community-based questionnaire in people who self-identified as trans in Canada,45 to 48.0% in a Belgian sample of trans sex workers44 and as high as 63% in urban groups of TW in New York City.46
Regarding BDNF:
Brain-derived neurotrophic factor (BDNF) is involved in neurogenesis, neuronal maturation and synaptogenesis, influencing brain plasticity. A study of 10 TW from Belgium showed a significant decrease in BDNF levels after 12 months of GAHT (p = 0.014) independent of age, weight, BMI, total fat mass, total lean mass, LH, FSH, oestradiol, testosterone, cortisol, physical activity or smoking.231Therefore, it was concluded that the decreased BDNF in TW after GAHT resulted from the GAHT rather than as a consequence of or risk factor for gender identity.231
This study is concerning given BDNF is important to brain health and function and is relevant to the aging process.
”Cross-sex hormone treatment in male-to-female transsexual persons reduces serum brain-derived neurotrophic factor (BDNF)” (Fuss et al., 2015)
Reduced serum BDNF in MtF thus seems to be a result of hormonal treatment rather than a consequence or risk factor of transsexualism.
Testosterone specific effects
Genital and pelvic pain are common with testosterone use.
Studies indicate testosterone use in trans-identified females indicates pelvic pain is the norm-
”Pelvic pain and persistent menses in transgender men” (Obedin-Maliver, 2016)
”Pelvic Pain in Transgender People Using Testosterone Therapy” (Zwickl, 2023) :
Results: Among 486 participants (median age = 27 years), 351 (72.42%) reported experiencing pelvic pain following initiation of testosterone therapy, described most commonly as in the suprapubic region and as ‘‘cramping.’’ Median duration of testosterone therapy was 32 months. Persistent menstruation, current or previous history of post-traumatic stress disorder, and experiences of pain with orgasm were associated with higher odds of pelvic pain after testosterone therapy.
In the same study also 63% reported painful orgasm; 58% pain during penetrative sex, and 31 % pain on touching external genitalia.
Severe clitoral pain is a known side effect of testosterone use in females:
“I Thought I Was Saving Trans Kids. Now I’m Blowing the Whistle”:
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
Thinning of the vaginal wall is another side effect for testosterone use in females. Also from the same article:
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
Testosterone significantly alters brain structures. While adult trans-identified females may desire these changes, it points to the fact that when tweens, teens, and young adults take testosterone, they may be altering the way their brain works and their personality significantly. And probably much more so, as brain development is not complete until age 25.
”Testosterone affects language areas of the adult human brain” (Hahn et al., 2016)
”Research shows testosterone changes brain structures in female-to-male transsexuals”
”Testosterone Effects on the Brain in Transgender Men” (Burke et al., 2018)
”The Effects of Testosterone on the Brain of Transgender Men” (Zubiaurre-Elorza et al., 2021)
”Gender-affirming hormonal treatment changes neural processing of emotions in trans men: An fMRI study” (Kiyar et al., 2020)
”Testosterone effects on functional amygdala lateralization: A study in adolescent transgender boys and cisgender boys and girls” (Becking et al., 2019)
Other side effects
Regarding the above study, a doctor wrote a letter to the editor and believed the researchers under reported the risk to females from testosterone induced erythrocytosis for political reasons. This is discussed for the general public in this Breitbart article, a paper with a conservative bias. But it is difficult to get more liberal leaning news sites to discuss risks:
Males and females have different laboratory ranges for hematocrit (red blood cells).
For adult men the range is 38.3 to 48.6 percent.
For adult women the range is 35.5 to 44.9 percent.
High testosterone levels can directly cause high levels of hematocrit.
Females who identify as trans males are given very high doses of testosterone to attempt to bring their testosterone levels into the male range.“Women who identify as trans males are being given very high, very risky doses of testosterone,” Laidlaw explained to Breitbart News about his concerns. “These high doses lead to high red blood cell counts. High red blood cell counts can lead to heart attacks and death. We believe these risks are being hidden.”
“Males and females have different normal ranges for red blood cell counts,” he elaborated. “We believe that the authors’ use of the male range for females hides a large number of females who will be at risk for heart disease and death.”
Laidlaw and colleagues, Andre Van Mol, M.D., Quentin Van Meter, M.D., and Jeffrey E Hansen, Ph.D., note results of the 1994 landmark Framingham study which showed “having high red blood cell counts (erythrocytosis) puts females at increased risk of cardiovascular disease, coronary heart disease and death due to both.”
“Studies of trans males have already shown up to a nearly five fold increased risk of myocardial infarction compared to females not taking testosterone,” the doctors explain at Gender Sanity…
The Swedish study, ”Lack of data hamper a proper toxicological risk assessment of the off-label use of testosterone in women with gender dysphoria” (Svens et al., 2021) summarizes the issues and calls for more research:

And:
Conclusions
Off-label use of testosterone in transmen has some unique characteristics, making it inherently riskier. High dose treatment is life-long and preclinical and clinical safety assessment studies performed for testosterone drugs lack the whole female group data as testosterone use is contraindicated in females due to teratogenicity. In addition, adverse effects related to off-label testosterone use in transmen is under-reported reported and is a possible patient safety risk. The lack of toxicology data would not be accepted for a new drug and the need for a comprehensive risk assessment is urgent.
Impacts on height
One goal of interfering with dysphoric youths’ natural puberty was likely to influence height to be more in line with the cross-sex identification. This area needs more research, but pediatric transition does not appear to achieve this. Puberty blocker use may stunt growth. In an interview with the Swedish journalist Carolina Jemsby, she states that some of the females who were put on puberty blockers were shorter than expected due to osteopenia.
Timing may be relevant because another study indicates they catch up when put on testosterone. T use in females may reverse stunted height due to puberty blockers and slightly increase an average for females. They will still, on average, be short for men and their bones stand a chance of being weaker than normal as the study below indicates.
”Just as Tall on Testosterone; a Neutral to Positive Effect on Adult Height of GnRHa and Testosterone in Trans Boys” (Willemsen, 2023)
We expect affirmative model doctors to start giving females human growth hormone, despite possible negative impacts. Doctors consider this for short youth as seen in the study below.
”Should Skeletal Maturation Be Manipulated for Extra Height Gain?” (Wit, 2021)
Puberty blockers do not appear to reduce male height. Starting them on puberty blockers earlier may cause them to be taller than they would have been. This negates justification for this practice on such young male children.
”Development of Hip Bone Geometry During Gender-Affirming Hormone Therapy in Transgender Adolescents Resembles That of the Experienced Gender When Pubertal Suspension Is Started in Early Puberty” (van der Loos et al., 2021)
Transgender Adolescents Resembles That of the Experienced Gender When Pubertal Suspension Is Started in Early Puberty (van der Loos et al., 2021):

Why would they be taller if they take puberty blockers early? Perhaps it is due to their influence on growth plates. This is from Australian guidelines, and they should not use the term female to describe biological males in medical literature. It’s purely ideological, confusing, and irresponsible:
Some trans females may also be distressed by linear growth beyond their expected final height due to delayed growth plate closure with oestrogen and testosterone deficiency.
However, the Dutch clinicians may use this study to justify puberty blocker use early merely because it influences the hip geometry to be closer to the opposite sex:
In both trans women and trans men, participants resembled the reference curve for SPW and ED of the experienced gender but only when GnRHa was started during early puberty. Those who started during mid and late puberty remained within the reference curve of the gender assigned at birth.
Another study indicates they may give them massive doses of estradiol because it slightly reduces height. One can see the results are very small, indicating this process cannot eradicate male genetics.
”Transgender Girls Grow Tall: Adult Height Is Unaffected by GnRH Analogue and Estradiol Treatment” (Boogers et al., 2020):
Results
Growth velocity and bone maturation decreased during GnRHa, but increased during GAHT. Adult height after regular-dose treatment was 180.4 ± 5.6 cm, which was 1.5 cm below PAH at the start GnRHa (95% CI, 0.2 cm to 2.7 cm), and close to target height (–1.1 cm; 95% CI, –2.5 cm to 0.3 cm). Compared to regular-dose treatment, high-dose estradiol and EE reduced adult height by 0.9 cm (95% CI, –0.9 cm to 2.8 cm) and 3.0 cm (95% CI, 0.2 cm to 5.8 cm), respectively.
Growth decelerated during GnRHa and accelerated during GAHT. After regular-dose treatment, adult height was slightly lower than predicted at start of GnRHa, likely due to systematic overestimation of PAH as described in boys from the general population, but not significantly different from target height. High-dose EE resulted in greater reduction of adult height than high-dose estradiol, but this needs to be weighed against possible adverse effects.
How do these hormones affect height? Growth will continue on PBs, but bone maturation slows due to a lack of sex hormones. But growth plate closure is delayed. When testosterone and estrogen are reintroduced, growth velocity increases and leads to bone maturation. If sex hormones are given in high doses (as is the case at gender clinics), it will quickly close growth plate growth. Genetics, human growth hormone (natural and prescribed), puberty blockers, and sex steroids can all influence height. Their interactions are very complicated and influenced by the timing of treatments. But overall, they have not proved this process significantly impacts more desirable height ranges.
Phalloplasty and Metoidioplasty
Both of these procedures (especially phalloplasty) have very high complication rates, with many being severe, even life-threatening. The study below covers some side effects of metoidioplasty, a surgery result that does not function like a male penis but is less risky than phalloplasty.
”Metoidioplasty Risks and Complications”
Stats from 2 studies-
Metoidioplasty: Surgical Options and Outcomes in 813 Cases (Bordas et al., 2021):
Follow-up ranged from 16 to 180 months (mean 94 months). Mean surgery time was 170 minutes and mean hospital stay was 3 days. Length of the neophallus ranged from 4.8 cm to 10.2 cm (mean 5.6 cm). Urethroplasty was complication-free in 89.5% of cases, and ranged between 81% to 90.3% in different groups. Urethral fistula and stricture occured in 8.85% and 1.70% of cases, respectively. Other complications included testicular implant rejection in 2%, testicular displacement in 3.20% and vaginal remnant in 9.60% of cases. From 655 patients who answered the questionnaire, 79% were totally satisfied and 20% mainly satisfied with the result of surgery. All patients reported voiding in standing position and good sexual arousal of the neophallus, without possibility for penetrative intercourse due to small size of the neophallus.
Overview on metoidioplasty: variants of the technique (Bizic et al., 2020):
Complications occurring after metoidioplasty are less frequent than in currently used phalloplasty techniques, ranging from 10 to 47% according to different literature data, and are mostly related to urethral reconstruction [12, 15, 24, 32].
Vaginoplasty
”Fancy a vaginoplasty? Think again” is an article discussing the lack of ethics and high complication rate of vaginoplasty:
I have seen horrific unethical practices by surgeons who lie about their experience and horrific results surgically as a result of that. We are using trans-gender people as guinea pigs and the medical profession allows this to happen,” said one doctor.
Other Surgeries
High complication rate with laryngoplasty-
”Gender-Affirming Laryngoplasty: Complications Relatively Common”
Cardiac/Circulatory Effects
There is not a complete picture in the literature regarding heart attack risk and strokes in people taking cross sex hormones. But evidence suggests there may be significant increased risks. From heart.org:
Previous research shows transgender men were almost 5 times as likely to report having a heart attack compared to cisgender women, those whose personal identity aligns with their sex at birth. Conversely, transgender women were more than 2 1/2 times more likely to have reported a heart attack than cisgender women – yet they did not have a significant increase in heart attack incidence when compared with cisgender men. However, a 2020 analysis found most of the studies examining gender-affirming hormones and blood pressure had sample sizes that were too small to detect statistically significant differences in blood pressure.
And from ”Hormone therapy for gender dysphoria may raise cardiovascular risks”:
The current study is the largest to date examining the cardiovascular risks of gender affirmation therapy in this historically understudied population. Previous research on hormone-modulating medications has primarily focused on younger women using hormone-based birth control or on older women following a hysterectomy or during menopause. In these populations, long-term hormone replacement therapy has been associated with an increased risk of breast cancer, stroke and blood clots…
In the study, people with gender dysphoria who had ever used hormone replacements saw nearly seven times the risk of ischemic stroke (a blockage in a vessel supplying blood to the brain), nearly six times the risk of ST elevation myocardial infarction (the most serious type of heart attack) and nearly five times the risk of pulmonary embolism (a blockage in an artery in the lung), compared with people with gender dysphoria who had never used hormone replacements. Hormone replacement therapy was not associated with any increase in deaths from any cause or with increased rates of atrial fibrillation, diabetes, hypertension, hemorrhagic stroke or heart failure.
Effects regarding reproductive cancers, fertility, and future offspring
Many trans-identified females want a hysterectomy to avoid pregnancy, breakthrough periods, and cancer risks. Little information is available regarding the impacts on fetuses. There are cases of females on T getting pregnant accidentally (sure to have hormonal influences on the fetus) and planning to get pregnant and stop testosterone.
”Endometrial findings among transgender and gender nonbinary people using testosterone at the time of gender-affirming hysterectomy” (Hawkins et al., 2021) indicates testosterone use affects the endometrial lining which may not revert if the female stops the testosterone use. Currently there appears to be no concern among affirmitve care providers regarding how this may impact babies via bith defects. Steroid use is known to cause them.
These researchers assert that “transphobia” contributes to pelvic pain due to testosterone use in the study “P088Uterine cramping and bleeding in transgender and nonbinary individuals on gender-affirming testosterone therapy” (Sobieraj et al, 2022).
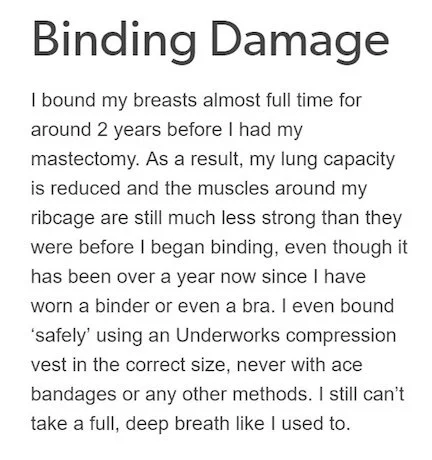
Mastectomy & Binding Side Effects
It appears that post-surgical pain is very common for double mastectomies.
From cancer.org:
Studies have shown that between 20% and 30% of women develop symptoms of PMPS after surgery. It's most common after operations that remove tissue in the upper outside portion of the breast or the underarm area.
Phantom breast sensation appears to be a side effect, according to the article ”The phantom breast after mastectomy, the homunculus and the hole in the cortical map.” (Dutta, 2015)
Binding is not safe, especially for the body of a growing adolescent, as demonstrated in the study ”Health impact of chest binding among transgender adults: a community-engaged, cross-sectional study” (Peitzmeier et al., 2015):
Over 97% reported at least one of 28 negative outcomes attributed to binding.
However, many “LGBTQ” youth websites promote, even celebrate the practice.
Extreme Body Modification for any Identity
The medical industry is becoming a service provider for what has turned into a capitalist body modification movement, but it is tax payers and insurance companies (paid for for all who have it) who will cover the expenses.
Outspoken and well-known affirmative model leaders such as Dr. Michelle Telfer are willing to put people on puberty suppression indefinitely for nonbinary identities. This case study involves a youth who identifies as nonbinary and has been on puberty blockers since age 11 and, at age 18, still wanted to be on puberty blockers. Doctors have kept this individual in a child-like, prepubertal state physically and likely mentally.
“Forever young? The ethics of ongoing puberty suppression for non-binary adults” (Notini et al., 2020) (emphasis ours):
Abstract
In this article, we analyse the novel case of Phoenix, a non-binary adult requesting ongoing puberty suppression (OPS) to permanently prevent the development of secondary sex characteristics, as a way of affirming their gender identity. We argue that (1) the aim of OPS is consistent with the proper goals of medicine to promote well-being, and therefore could ethically be offered to non-binary adults in principle; (2) there are additional equity-based reasons to offer OPS to non-binary adults as a group; and (3) the ethical defensibility of facilitating individual requests for OPS from non-binary adults also depends on other relevant considerations, including the balance of potential benefits over harms for that specific patient, and whether the patient’s request is substantially autonomous.
Hormones, particularly estrogen, are critical for bone density. As people enter their thirties, bone density begins to decrease. If kept on puberty blockers, this person will be at risk for weakened bones and fractures. Many other areas of the body require a normal balance of hormones for healthy function, and what are healthy levels are sex-specific.
The later part of the abstract demonstrates that gender medicine is a product provided based on the patient demands. This removes guard rails to protect people from medically assisted self-harm. Failure to adhere to these ethics has led to unnecessary cosmetic surgery by people with body dysmorphic disorder and widespread opiate addiction.
Although the broadly principlist ethical approach we take can be used to analyse other cases of non-binary adults requesting OPS apart from the case we evaluate, we highlight that the outcome will necessarily depend on the individual’s context and values. However, such clinical provision of OPS should ideally be within the context of a properly designed research study with long-term follow-up and open publication of results.
Other studies regarding this subject-
”Partial Gender-Affirming Hormone Treatment in Non-Binary Transgender Individuals in a Referral Center Cohort” (Van Dijken et al., 2021)
”Selective Estrogen Receptor Modulators: A Potential Option For Non-Binary Gender-Affirming Hormonal Care?” (Xu et al., 2012):
Here, we discuss the theoretical use of Selective Estrogen Receptor Modulators (SERMs) for non-binary people assigned male at birth (AMAB) who are seeking an androgynous appearance through partial feminization without breast growth.
Case reports
”Androgen-receptor-positive hepatocellular carcinoma in a transgender teenager taking exogenous testosterone” (Lin et al, 2020)
”Implications for management of ovarian cancer in a transgender man: Impact of androgens and androgen receptor status” (Aubrey et al., 2021)
”Case Report: Invasive Endometrial Cancer in a Trans Man and Risk of Testosterone Therapy” (Jeevananthan et al., 2021)
”Management of Recurrent Deep Vein Thrombosis in a Transgender Woman” (Oguz et al., 2021)
Conclusion
Corinna Cohn, is a trans-identified person who discusses gender and other issues on the Heterodox podcast. This statement provides a good sumation of the longterm risks and challenges that young people who medicalize will face.
